
Not Our Future, Bob Moran, bobmoran.co.uk
|
Imagine running out of imagine
Mistaking authority for power Weaving lifes free spirit Into patterns of control |
In the reality
Of many realities How we see what we see Affects the quality Of our reality |
| Nov 2020: | Apprehending the False Promise of Biosecurity |
| Unmasking Usurpation by Fear Merchants | |
|
Oct 2021: | Conscience and The Nuremberg Code |
| Informed Consent, Censorship, and Inalienable Rights |
The intent of assembling this witness is to encourage renewing the bond each of us has with our Creator and revisiting life questions as Peter d’Errico frames it in Seeing Between Worlds: “What are we here for? What does it mean to be human? What is my relation to everything and everyone else?”
Our intelligence. Now whoever it is we pray to, right?, whoever it is we pray to, however we pray, whatever, however we do that, alright?, I think that we have an obligation and a responsibility and it’s about respect. If we respect our Creator, then we should use our intelligence as intelligently as we can as often as we can. And that means with clarity and coherence. That means to activate and respect our intelligence and activate the thinking process so that it’s going the way we want it to be because that’s why it was given to us. Our intelligence – as the human being part of all of this reality that’s going on, we were given intelligence, this is what was there to help us through the evolutionary reality – to ride the balance, so to speak, of the evolution with our intelligence. It’s our medicine, it’s our protection, it’s our self-defense. Those fears and doubts and insecurity in one’s daily mind and reality – how much do they affect one’s daily mind and reality? How much do they affect the ones of the people around them that they’re connected to and that they care about? What’s the repercussions of the fears and the doubts and insecurity? Because I guarantee you, every day when we get up, we use our intelligence to create those effects. So it isn’t that we’re not using our intelligence, or we can’t use our intelligence – we can’t stop using our intelligence. But it’s about as human beings, taking the responsibility to be as clear as one possibly can be about it and use our intelligence the way our Creator gave it to us to use.—John Trudell, What It Means To Be A Human Being, 2001
|
“
|
Money = power and power = money is the supreme religion of our age. The high priests of this church are extolled in such venues as Forbes World’s Billionaires List - The Richest in 2022: The number of billionaires on Forbes’ 36th annual list of the world’s wealthiest are 2,688. As a ratio, the current 2,688 moguls make up 0.0000003 percent—or one “priest” per 2,976,190 humans—of the
8+ billion souls now on Mother Earth. The influence this religious cult exerts managing and directing the perceptions of humanity serves one of the oldest time-proven strategies for power and control: divide and conquer. Consider: today’s largest global investment corporations are Blackrock [†][††] and Vanguard. As of November 2022, Vanguard has more that $8.10 trillion assets under management (AUM), second to Blackrock, Inc with $9.57 trillion AUM. These two firms combined own The New York Times Corporation, other legacy media, and Big Pharma.
|
In 1996, E. Martin “Marty” Schotz self-published History Will Not Absolve Us: Orwellian Control, Public Denial, and the Murder of President Kennedy. Its incisive focus on the assassination of the 35th President “in a conspiracy organized at the highest echelons of power in Washington” “reveals the Orwellian techniques by which the public has allowed itself to be led into confusion about the assassination and assembles the documentary evidence necessary to know without a doubt who killed President Kennedy and why.” (See the nonpareil work of Jim Douglass, Vincent Salandria, and Marty Schotz to know without a doubt who killed President Kennedy and why.)
Today in 2022, the Orwellian techniques by which the public has allowed itself to be led into confusion about what constitutes “Pubic Health,” informed consent, freedom of thought and speech, and human dignity, are revealed in the unprecedented global, experimental medical intervention and integral censorship program smothering all perspectives not conforming to the single, all-encompassing one-size-fits-all official narrative.
While the actual facts involving the assassination of President Kennedy might not seem relevant today, official government statements, echoed and reinforced in corporate state press organs, indicate otherwise. Take the following, from the 10 June 2022 Boston Globe, page 1 headline, ‘The world is watching’: Jan. 6 evidence tells the story, by Luike Broadwater, New York Times, page A5:
The assertion of integrity in “landmark fact-finding committees” including the Kennedy assassination, is beyond ludicrous. And yet, who benefits by this class of statements that are continually trotted out as uncontested facts? Certainly not the 99% of humanity that this perception management operation is directed at.
Pre-eminent journalist, investigator, and author Gaeton Fonzi spoke in 1993 about Getting Slapped In The Face By US Intelligence Over and Over and Over Again – When Will We Wake Up? At one point he referred to Mr. Schotz’s observation that,
“It is so important to understand that one of the primary means of immobilizing the American people politically today is to hold them in a state of confusion in which anything can be believed but nothing can be known, nothing of significance that is.
“And the American people are more than willing to be held in this state because to know the truth—as opposed to only believe the truth—is to face an awful terror and to be no longer able to evade responsibility. It is precisely in moving from belief to knowledge that the citizen moves from irresponsibility to responsibility, from helplessness and hopelessness to action with the ultimate aim of being empowered and confident in one’s rational powers.”
So Marty Schotz is absolutely right. Today most Americans BELIEVE there was a conspiracy to kill President Kennedy, but they don’t KNOW it. They don’t want to KNOW it—and our government doesn’t want to KNOW it and our elected representatives don’t want to KNOW it because KNOWING it would mean having to do something about it. That’s an awesome thought.
Decades later, we are living in period of 2.5 years and counting where many people continue to believe “the pandemic” is so uniquely dangerous that the cancellation of a vast array of inalienable rights is appropriate and necessary. What has been dictated from on high—lockdowns[†][††], chronically misused testing, masks, social (note: not physical) distancing, blackout of strikingly effective repurposed drugs and therapies keeping people out of hospital and recovering from illness, and the terrifying, unspeakable toll of injuries and death from experimental injections—has been effected by the concerted, singular playbook carried out almost universally around the globe. The corresponding suppression of the actual consequences of this watershed catastrophe in the history of our species has made it possible for people to evade knowing what has occurred. Hence the ultimate good of being empowered and confident in exercising one’s rational powers has been effectively cut off by the broken-record drumbeat of falsehoods and untruths buttressed by the suffocation of empirical knowledge demonstrating the hollow claims for what they are: lies, obfuscations, omissions and distortions.
In 2018 James Tracy assembled The CIA and the Media: 50 Facts the World Needs to Know in which are presented “historical and contemporary facts—by no means exhaustive—provid[ing] a glimpse of...the power such entities possess to influence if not determine popular memory and what respectable institutions deem to be the historical record.”
|
“
|
Thousands of years old, Divide and Conquer has kept our species—our unitary single human family we all belong to—separated and fragmented within false divisions: male against female, young against old, "black"-"red"-"yellow"-"white" against "white"/"yellow"/"red"/"black", "left" against "right", "democrat" against "republican", "conservative" against "liberal", one faith against another, "vaxed" against "unvaxed" ... How many separations can you name and identify? What about rich against poor? Is that the same divide? Think feudalism, the Doctrine of Discovery, colonialism, slavery, imperialism.
|
|
—David Ratcliffe, Coda, Conscience and the Nuremberg Code, 19 Oct 2021
|
|

The etymology of the verb, expropriate, is “to hold no longer as one’s own, give up a claim to the exclusive property of”. Such ideas as democracy, constitutional rights, and even human dignity have been increasingly debased over time. The collapse of structures and systems constituting the Industrial Age are increasingly apparent as we travel further into the 21st century.
Many people who began learning to think critically in their younger school years identified foundations of this ongoing dis-integration decades ago. In Four Arguments for the ELIMINATION of Television (1977), Jerry Mander analyzed the Expropriation of Knowledge and how, “as we continue to separate ourselves from direct experience of the planet, the hierarchy of techno-scientism advances”:
At the moment when the natural environment was altered beyond the point that it could be personally observed, the definitions of knowledge itself began to change. No longer based on direct experience, knowledge began to depend on scientific, technological, industrial proof.
Scientists, technologists, psychologists, industrialists, economists and the media which translate and disseminate their findings and opinions became our source. Now they tell us what nature is, what we are, how we relate to the cosmos, what we need for survival and happiness, and what are the appropriate ways to organize our existence.
There is little wonder, therefore, that we should begin to doubt the evidence of our own experience and begin to be blind to the self-evident. Our experience is not valid until science says it is. (Mother’s milk is healthy!)
It is also little wonder that we feel removed from participation in the larger issues which shape our lives. We feel removed because we are removed.
As we continue to separate ourselves from direct experience of the planet, the hierarchy of techno-scientism advances. This creates astounding problems for a society that is supposed to be democratic.
In democracies, by definition, all human beings should have a say about technological developments that may profoundly change, even threaten, their lives: nuclear power, genetic engineering, the spread of microwave systems, the advance of satellite communications, and the ubiquitous use of computers, to name only a few. And yet, in order to participate fully in discussions of the implications of these technologies one must have training in at least physics, psychology, biology, philosophy, economics, and social and political theory. Any of these technologies has profound influence in all those areas. Because most of us are not so trained, all discussion takes place among our unelected surrogates, professionals and experts. They don’t have this full range of training either, but they do have access to one or another area of it and can speak to each other in techno-jargon—“tradeoffs,” “cost-benefits,” “resource management”—and they therefore get to argue with each other over one side of the question or the other while the rest of us watch.
That their technological training and the language they use excludes from their frame of reference a broader, more subtle system of information and values rarely seems to occur to them.
The alternative to leaving all discussion to the experts would be to take another route entirely. That would be to define a line beyond which democratic control—which is to say full participation of the populace in the details of decisions that affect all of us—is not possible, and then to say that anything which crosses this line is taboo. Yet, the notion of taboo is itself taboo in our society, and the idea of outlawing whole technologies is virtually unthinkable.
San Francisco ecologist Gil Baillie, in a brilliant article in the 1975 edition of Planet Drum, argues that taboo systems of earlier cultures were not quite the darkly irrational frameworks we now believe them to have been. Most often they reflected knowledge taken from nature and then modified by human experience over time. Their purpose was to articulate and preserve natural balances in a given area or within a given group of people at a particular time. They were statements about when too far is too far. This sensitivity to natural balances, which was the basis of virtually every culture before our own, has now been suppressed by our modern belief that science and technology can solve all problems and that, therefore, all technologies which can be created ought to be. The question of natural balance is now subordinated. Evolution is defined less in terms of planetary process than technological process. The planet and its information are now considered less relevant than human ingenuity, an idiotic and dangerous error shielded from exposure only by the walls of previous assumption and the concrete of the physical forms within which we live.
Ivan Illich, a leading critic of the expropriation of knowledge into a nether world of experts and abstraction, argues in Medical Nemesis that professional medicine may be causing more harm than good. We go to doctors as we go to mechanics. They speak a language that remains impenetrable to us. We take their cures on faith.
Illich remarks that this may be producing more illness than cure: It has separated people from knowledge about keeping themselves healthy, a knowledge that was once ingrained in the culture. Although some of our techno-scientific methods work, some do not, and the doctors who use them may not understand them or may be inexpert in their use. The doctors, Illich believes, are also taking the validity of techno-medicine on faith. Their source is usually the chemical and drug industry, which has a stake in disrupting natural healing methods. How else could they sell their chemicals?
Mander’s understanding of and appreciation for the supreme value of sensitivity to natural balances and recognizing the wisdom of when too far is too far is evermore needed now, 4-plus decades hence. His expressly calling out the idiotic and dangerous error of thinking the planet and its information are less relevant than human ingenuity harkens back to the downfall of ancient Greece where hubris—overweening pride and arrogance—drives humans to follow paths and projects leading to self-destruction.
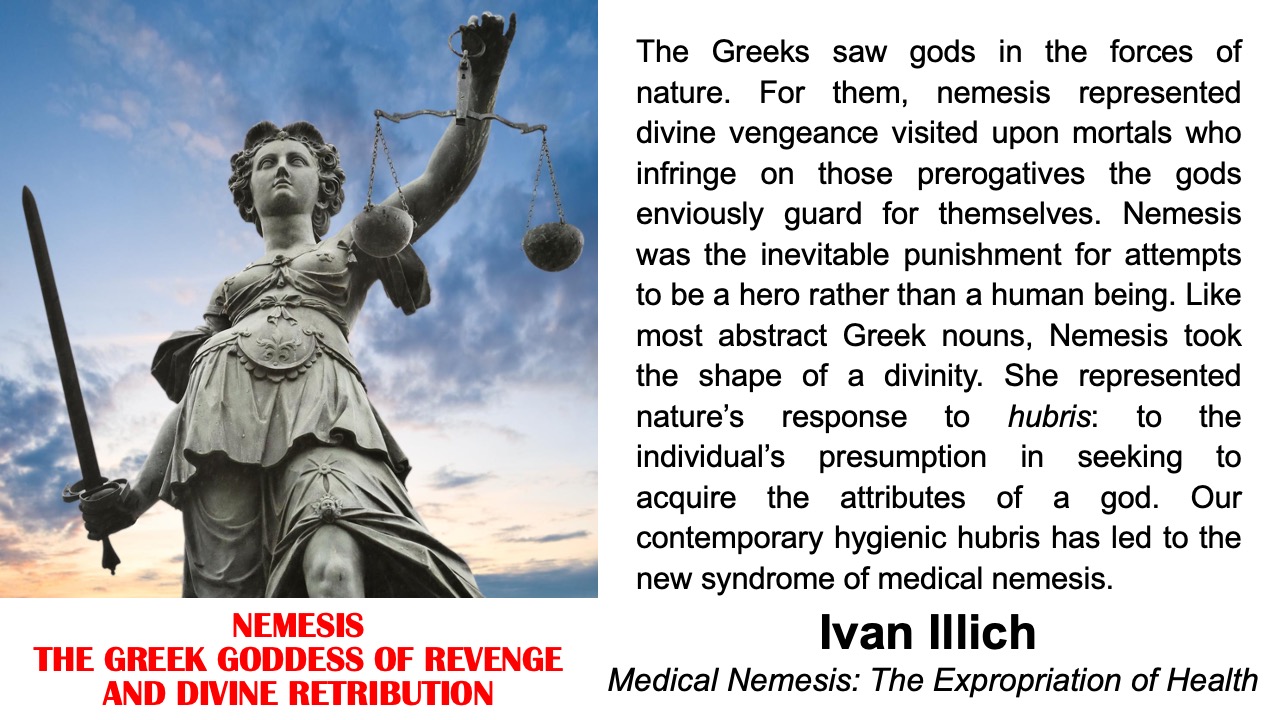
In his own words, “trained as a medieval historian and philosopher” and who taught “about the history of friendship and the history of the art of suffering”, Ivan Illich wrote about The Medicalization of Life in Medical Nemesis: The Expropriation of Health. First published in 1974, the Introduction leads off with, “The medical establishment has become a major threat to health. The disabling impact of professional control over medicine has reached the proportions of an epidemic. Iatrogenesis, the name for this new epidemic, comes from iatros, the Greek word for ‘physician,’ and genesis, meaning ‘origin.’”
In Chapter 2, The Medicalization of Life, Illich observes how “The higher the price tag at which well-being is commandeered, the greater will be the political prestige of an expropriation of personal health.”
In the final Chapter, The Recovery of Health, The Right to Health calls for a halt to the expropriation of every person’s coping ability and presents an alternative to the inevitable Medical Nemesis that will set in unless the autonomy of the individual is re-established.
Increasing and irreparable damage accompanies present industrial expansion in all sectors. In medicine this damage appears as iatrogenesis. Iatrogenesis is clinical when pain, sickness, and death result from medical care; it is social when health policies reinforce an industrial organization that generates ill-health; it is cultural and symbolic when medically sponsored behavior and delusions restrict the vital autonomy of people by undermining their competence in growing up, caring for each other, and aging, or when medical intervention cripples personal responses to pain, disability, impairment, anguish, and death.
Most of the remedies now proposed by the social engineers and economists to reduce iatrogenesis include a further increase of medical controls. These so-called remedies generate second-order iatrogenic ills on each of the three critical levels: they render clinical, social, and cultural iatrogenesis self-reinforcing.
The most profound iatrogenic effects of the medical technostructure are a result of those nontechnical functions which support the increasing institutionalization of values. The technical and the nontechnical consequences of institutional medicine coalesce and generate a new kind of suffering: anesthetized, impotent, and solitary survival in a world turned into a hospital ward. Medical nemesis is the experience of people who are largely deprived of any autonomous ability to cope with nature, neighbors, and dreams, and who are technically maintained within environmental, social, and symbolic systems. Medical nemesis cannot be measured, but its experience can be shared. The intensity with which it is experienced will depend on the independence, vitality, and relatedness of each individual.
The perception of nemesis leads to a choice. Either the natural boundaries of human endeavor are estimated, recognized, and translated into politically determined limits, or compulsory survival in a planned and engineered hell is accepted as the alternative to extinction. Until recently the choice between the politics of voluntary poverty and the hell of the systems engineer did not fit into the language of scientists or politicians. Our increasing confrontation with medical nemesis now lends new significance to the alternative: either society must choose the same stringent limits on the kind of goods produced within which all its members may find a guarantee for equal freedom, or society must accept unprecedented hierarchical controls[endnote 3: The Honorable James McRuer, Ontario Royal Commission Inquiry into Civil Rights (Toronto: Queen’s Printer, 1968, 1969, 1971). On self-governing professions and occupations, see chap. 79. The granting of self-government is a delegation of legislative and judicial functions that can be justified only as a safeguard to public interests.] to provide for each member what welfare bureaucracies diagnose as his or her needs. [emphasis added]
The articulation of nemesis leading to a choice of defining natural boundaries to human endeavors echoes Mander’s expression of taking an entirely different route than leaving all discussion to the experts. As well, the “new kind of suffering” described 45 years ago—anesthetized, impotent, and solitary survival in a world turned into a hospital ward—is frighteningly prescient in terms of people being “largely deprived of any autonomous ability to cope with nature, neighbors, and dreams and who are technically maintained within environmental, social, and symbolic systems.”
Of the three levels of iatrogenesis Illich defines and describes—clinical, social, and cultural— beyond the first two, today’s upside-down world is being forced into an unprecedented cultural and symbolic medical chamber of horrors “when medically sponsored behavior and delusions restrict the vital autonomy of people by undermining their competence in growing up, caring for each other, and aging, or when medical intervention cripples personal responses to pain, disability, impairment, anguish, and death.”
Illich’s framing of nemesis in terms of “our contemporary hygienic hubris” is a life-affirming beacon, illuminating what we are collectively in danger of losing, possibly forever.
The Greeks saw gods in the forces of nature. For them, nemesis represented divine vengeance visited upon mortals who infringe on those prerogatives the gods enviously guard for themselves. Nemesis was the inevitable punishment for attempts to be a hero rather than a human being. Like most abstract Greek nouns, Nemesis took the shape of a divinity. She represented nature’s response to hubris: to the individual’s presumption in seeking to acquire the attributes of a god. Our contemporary hygienic hubris has led to the new syndrome of medical nemesis.[endnote 73: The term was used by Honoré Daumier (1810-79). See reproduction of his drawing “Némésis médicale” in Werner Block, Der Artzt und der Tod in Bilden aus sechs Jahrhunderten (Stuttgart: Enke, 1966).]
By using the Greek term I want to emphasize that the corresponding phenomenon does not fit within the explanatory paradigm now offered by bureaucrats, therapists, and ideologues for the snowballing diseconomies and disutilities that, lacking all intuition, they have engineered and that they tend to call the “counterintuitive behavior of large systems.” By invoking myths and ancestral gods I should make it clear that my framework for analysis of the current breakdown of medicine is foreign to the industrially determined logic and ethos. I believe that the reversal of nemesis can come only from within man and not from yet another managed (heteronomous) source depending once again on presumptious [sic] expertise and subsequent mystification.
Medical nemesis is resistant to medical remedies. It can be reversed only through a recovery of the will to self-care among the laity, and through the legal, political, and institutional recognition of the right to care, which imposes limits upon the professional monopoly of physicians. [emphasis added]
The medical nemesis our single, supremely gifted human family is confronted with today threatens further evolution of the creative spark to explore what the nature of being human means, bestowed as birthright to all now alive and all that come after us.

In a November 2000 interview with John Judge, I began by citing a letter he wrote to me four days before that year’s Presidential election:
Bush will win the election—it was pre-decided. It’s simple logic to me. If they spend $10 million to rig elections in Chile, what will they spend here, where it counts? They can’t leave it up to chance. How is it rigged?Electoral college just in case, funds necessary to run eliminating all but the super rich and those they pick, framing of the race by “polls” who say in advance who “cannot win”, betting both horses in the race, exit poll and other factors to influence votes, control of the “issues” and the nature and range of the debate, and rigging of the computerized tallying (Vote Scam) if needed, discouragement from voting so that a very few elect one of the pre-chosen evils. For the model, see Ed Herman’s Demonstration Elections and realize that what we do abroad we have to do here even more urgently. And the last controls: bribe, bully, blackmail or bullet. Put Clinton over the Monica barrel and make him bomb Kosovo for instance.
Pre-decided because we had our breathing space but now they will take off the glove and bring down the iron fist. The wealth is so concentrated now that they cannot afford the illusions of either social supports or democratic options. Seattle, Philly and DC were early warning signs about the increased role of the military and brutal police response in popular control.
In stages since 22 November 1963, the glove has come off the iron fist. From the double-barrel September 2001 bombings followed by the Anthrax Deception[†][††], to the upside-down world humanity is being relentlessly dragged into since early 2020, we are now confronted with a global Spiritual War of previously-incomprehensible dimensions. The initial sphere of operations in this war is medical nemesis. As Ivan Illich stated, “Medical nemesis is resistant to medical remedies.”
In March 2020 the new mantra inaugurating the Biosecurity State was unveiled with the incantation: Two Weeks To Flatten The Curve. As an act of enchantment, uttering magical words replete with ceremonies imbued with magical power, this incantation initially succeeded in a global lockdown beginning an unprecedented experiment in medical and political history. The threshold breached turned weeks into years with the consequent, ongoing bid to expropriate inalienable rights in service to the stay safe meme. Benjamin Franklin warned of this devil’s bargain when he wrote, “Those who would give up essential Liberty, to purchase a little temporary Safety, deserve neither Liberty nor Safety.” George Carlin channeled Ben Franklin in 1999 on this, leading off with “it’s just one more way of reducing your liberty...”.
In May 2020, Giorgio Agamben wrote a short piece on Biosecurity and Politics. Containing many cogent observations about “what is at stake is a new paradigm for the governance of men and things”, Agamben observed:
It is evident that, apart from the emergency situation, linked to a certain virus that may in the future be replaced by another, at issue is the design of a paradigm of governance whose efficacy will exceed that of all forms of government known thus far in the political history of the West. If already, in the progressive decline of ideologies and political beliefs, security reasons allowed citizens to accept limitations on their liberty that they previously were unwilling to accept, biosecurity has shown itself capable of presenting the absolute cessation of all political activity and all social relations as the maximum form of civic participation.While there is an appearance of a return to political activity, the range of allowable discourse is tenaciously controlled and limited by big tech, corporate state media, 24/7 fear programming by government officials, and academic and medical “experts”. Cases in point are five ultimate confrontations with medical nemesis:
Combined, these five elements form the nexus of the developing Biosecurity State. The single, official corporate state narrative dominating print, broadcast, and digital venues endeavors to dismiss and stamp out all public debate and any perspective that runs counter to this through omission, distortion, lack of contextual analysis, and disinforming opinion stated as obvious, incontestable fact.

The good news here is the rising tide of an incredible motherlode of independent voices challenging the sanctioned story of what is occurring with penetrating intelligence, wide-ranging wisdom, and inspired critical analysis. Ever-growing multitudes of Medical Doctors and Scientists, Virologists, Epidemiologists, Pathologists, Physicists, Attorneys, Paralegals, Professors, Authors, Statisticians, Economists, and Playwrights—some of whom also comprise “Journalists The Next Generation” in the here-and-now picking up the banner of what was The Fourth Estate—are collaboratively producing rubber-meets-the-road independent analysis and cogent, incisive evaluation of how our world is actually operating. These voices are the sacred antidote to the Orwellian crimestop seeking absolute control to silence all independent reasoning and are celebrated in what follows. Listings of some of these souls include Credentialed Experts in @JustCallMeJack’s Totality of Evidence and many at CAMPFIRE WIKI including Pandemic Related Must Read Substacks.
|
“
|
Your Congressmen, Senators, School Boards, Employers, health departments and your friends and family deserve to know and understand that their RT-PCR test results - and those of their loved ones - may, in fact, be incorrect, and that the CDC protocol has an unacceptably high false discovery rate. Isolation due to false positives is disruptive, caused mass chaos in all sectors of society, and false positives gave - and are still giving - individual patients a misunderstanding of their immune and infectious status.
Dr. Lee’s earlier published study showing false negatives in the nonQ-RT-PCR designated technical samples also means that people have been testing negative for SARS-CoV-2 infection when, in fact, they had a SARS-CoV-2 virus infection.
Dr. Lee, Dr. Lyons-Weiler, and Dr. Ealy tried in earnest to tell the FDA and CDC all of this would happen. They were able to see the most fundamental details of mass-testing, and, as a result, the cost to society has been immeasurable.
The response by CDC was to lower the Ct threshold for case determination in the vaccinated in May of 2021, but to continue biasing the unvaccinated case count upward using arbitrarily high Ct threshold values in the unvaccinated.
It’s time to demand accountability and bring public health to heel, answerable to elected, not appointed officials.
| |
|
—James Lyon-Weiler, Peer-Reviewed Study Confirms Fatal Flaw in PCR Testing, Popular Rationalism, 31 Oct 2022
|
||

The term “vaccine” is used here with qualification. In the past, the definition of “vaccine” included “A product that stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from the disease.” In 2021 this was altered, removing “stimulates a person’s immune system to produce immunity” to now state, “A preparation that is used to stimulate the body’s immune response against diseases.” The 2015 WHO document, “Module 2: Vaccines and drugs: similarities and differences,” cites the old CDC vaccine definition.
The GAO report on Operation Warp Speed (Feb 2021) opens with: “The Coronavirus Disease 2019 (COVID-19) pandemic has resulted in catastrophic loss of life and substantial damage to the global economy, stability, and security.” The official narrative’s claim of catastrophic loss of life due to the lethality of the SARS-CoV-2 virus is based on categorical misuse of what the CDC branded as the “Gold Standard” diagnostic tool: the reverse transcriptase-polymerase chain reaction or RT-PCR test. Kary Mullis, inventor of the PCR test, was very clear about it being designed as a manufacturing technique—not as a diagnostic tool. As Dr. Byram Bridle evaluated this in cogent detail, “Misuse of An Elegant Scientific Technique Has Plagued COVID-19 Science From the Very Beginning.” In this way, mis-informing/dis-informing data pronouncements by government officials and medical experts created an extremely dangerous false narrative about the lethal nature of SARS-CoV-2 and counting deaths from Covid.
The risks and consequences of the one-size-fits-all experimental vaccines still in phase three clinical trials being imposed on humanity and sanctioned by the Emergency Use Authorization, are EXHIBIT NUMBER 1 in the expropriation of personal health and inalienable rights, purportedly for the purpose of staying safe. However, the actual accumulating data from the injections begun in December 2020, reveal unconscionable injury, trauma, suffering, and death. There are expanding mountains of research and studies, reports, data analyses, essays, articles, presentations, and more detailing the fallout from these phase three clinical trial injections.
In 1976 there were less than 50 deaths from inoculations for the Swine Flu before that program was halted.
A key to understanding how this happened is the 400,000 pages of documents pertaining to the approval under the Emergency Use Authorization of Pfizer’s C19 Vaccine for ages 16-plus.
After the FDA approved the Pfizer shot marketed as Comirnaty on 23 Aug 2021, Public Health and Medical Professionals for Transparency (PHMPT)—made up of public health and medical professionals, scientists, and journalists—submitted a Freedom of Information request to the FDA for all data within Pfizer’s C19 vaccine biological file. PHMPT’s sole purpose is to make the biological product files data publicly available for each of the C19 vaccines, enabling independent review and analyses, starting with Pfizer.
The FDA tried to lock this data away from public discussion and evaluation for 75 years. PHMPT then sued the FDA for not releasing the data and on 2 Feb 2022 Federal Judge Mark Pittman ordered the FDA to release redacted versions of the documents. Pfizer documents began being released in November 2021 and starting that December are released in batches at the beginning of each month at: phmpt.org.
One illustration: an initial release of Pfizer post-marketing data from December 2020 to February 2021 is titled, 5.3.6 Cumulative Analysis of Post-authorization Adverse Event Reports. Pfizer was well aware of the risks and consequences of its shots: 1,223 people died in the first 90 days of injections and 1,284 medical injuries were registered in Appendix 1. List Of Adverse Events Of Special Interest filling the last nine pages of this document [see Appendix 2]. No wonder the FDA wanted to bury the 400,000 pages of Pfizer EUA documents for 75 years.
Concerning pregnancy outcomes in the above document, Pierre Kory, MD, MPA, wrote an analysis on 20 Aug 2022:
Too many young people dying, too many becoming disabled, too many pregnancies resulting in fetal or neonatal death as above, and now we find out that if we continue with this vaccine obsession, they will not be replaced. This is a humanitarian catastrophe heaped atop the one caused by dangerous gain-of-function research. When will the world wake up to this rapidly unfolding horror? For those of us who know what is going on, it is hard not to feel helpless as we are forced to watch increasingly apparent and widespread needless death. But we will continue to try to get these truths out despite the massive censorship and propaganda overwhelming the globe. We have a moral and ethical obligation and take that responsibility seriously no matter what befalls us. Stop the vaccines, now. And if we can’t stop them, we must try to convince everyone we know to no longer agree to get vaccinated. Their lives and our future depend on it.
The above hyperlink to widespread needless death goes to a post by NYU Professor Mark Crispin Miller. I have been producing an ongoing, updated listing, from its beginning in February, of Mark’s reporting of “In Memory of Those Who Have ‘Died Suddenly’”. The ongoing, expanding “roll call” enumerated in this is beyond grotesque, beyond unthinkable, given that NO MSM journalist/writer/reporter/broadcaster will shout from the rooftops what is happening here. As Crispin Miller summarizes the situation:
In other words, “died suddenly,” and “died unexpectedly,” though still used in that former coded way, are now frighteningly apt descriptors of how people everywhere, and of all ages, have been passing on abruptly, here one moment and gone the next, though in ostensibly good health.
Finally, in putting out these compilations I have also noted often that, while all too many have “died suddenly” for no reported reason, many others have been felled by either cardiological mishap—heart attack, stroke, blood clots, cardiac arrest—or sudden aggressive cancers: two categories of fatal illness that are now both well-established as “adverse events” post-“vaccination.” This too is entirely new, especially when it comes to countless children “dying suddenly” of “massive” heart attacks, which, once upon a time, was as unusual as children dying of COVID in 2020.
Take just 5 MINUTES to pan through the global account for the beginning of December. Note the increasing number of young, healthy people suddenly dying. The absolute horror of these people’s lives being extinguished calls ALL who can “face the music” to honor their memories and the grief of their families and friends by finding ways (some of which are described below) to help STOP this annihilation madness.
On 14 Jul 2022 Kruse Law in Switzerland filed a Criminal Complaint against Swissmedic. Concerning Swissmedic, as stated in paragraph 3 of the Executive Summary, “it has the central function of protecting the health of the Swiss population.” The stated motivation for publishing this criminal complaint is the health hazard: “We are dealing here with nothing less than the greatest danger – indeed, injury – to human health that has ever occurred in Switzerland.” Paragraph 142 on Page 124 of the 302-page Criminal Complaint presents the staggering increase in athletes who have died suddenly: the monthly average from 1996 to 2004 was 2.35 athlete deaths; from Jan 2021 to April 2022 it was 42 athlete deaths.
Worldwide, reports about the connection between “vaccination” and myocarditis are increasing: even in a study conducted for the CDC and FDA, scientists came to the conclusion that the upper limit of the expected myocarditis rates had been significantly exceeded, especially in young men and women. This is also evident worldwide in the many young athletes who collapse “suddenly and unexpectedly” (on the playing field). Since the start of the vaccination campaign at the beginning of 2021 until 24 June 2022, 14,013 medical incidents and “sudden deaths” have been recorded internationally among professional and amateur athletes. The average age of these cases was 40 years. This is clearly not something that would have always existed, but an entirely new development. For example, the number of athletes who died suddenly has apparently increased massively compared to previous years:There is so much about this situation that is deafening. Yet not a peep is being acknowledged by so-called authorities who have the power and the position to call FULL STOP so that a thorough, independent accounting of the consequences of the C19 Vaccines is conducted—and then the results are acted upon. On 2 Sep 2022 Steve Kirsch published an incredibly damning piece: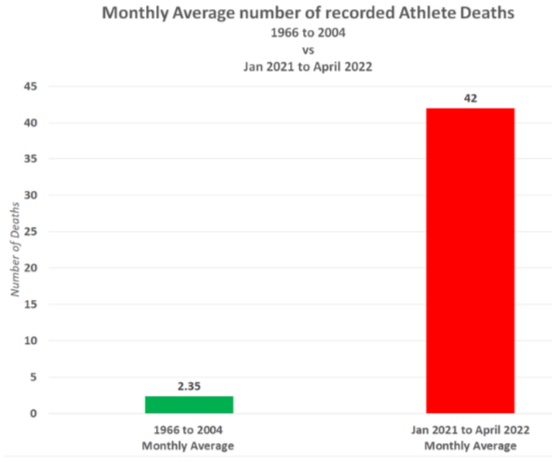
Michael Palmer MD and Sucharit Bhakdi MD are members of Doctors for COVID Ethics, “doctors and scientists from 30 countries, seeking to uphold medical ethics, patient safety, and human rights in response to COVID-19.” Two recent, jointly written articles analyze some of the serious adverse effects of the C19 vaccines:There is yet another signal that there is a 5 month “time bomb” fuse after vaccination which is the “blood clots” (which are not blood). Read this article about these clots. I’ve written many articles about the clots which are found in up to 93% of the cases. Jessica Rose wrote an excellent article explaining how these clots form.
These clots take months to form before they kill you. The embalmers didn’t see any of these clots until mid-2021. This suggests there is a double spike of death, just as Tim Ellison found. There is a quick death: these are the ones reported in VAERS. And there is the slower death from the clots that take, on average, about 5 months to kill you. This explains why none of the embalmers noticed any of these cases until mid-2021.
mRNA vaccines against COVID-19 and their effects on the central nervous system, 2 Oct 2022
This article summarizes evidence from experimental studies and from autopsies of patients deceased after vaccination. mRNA vaccines travel throughout the body and accumulate in various organs and induce long-lasting expression of the SARS-CoV-2 spike protein in many organs. The vaccine-induced expression of the spike protein induces autoimmune-like inflammation, which can cause grave organ damage, especially in vessels, sometimes with deadly outcome.
Vascular and organ damage induced by mRNA vaccines: irrefutable proof of causality, 19 Aug 2022
There are numerous case reports of central nervous system disorders following the use of mRNA vaccines against COVID-19. These disorders include stroke, cerebral hemorrhage, and encephalitis. It is not necessary for the vaccines to cross the blood-brain barrier to harm the brain; however, this must be considered possible, especially after repeated injections or accidental intravenous injection, and it is likely to aggravate the clinical course of encephalitis.
One US Senator, Ron Johnson (R-Wis), has steadfastly worked to bring oversight and transparency to USG policy concerning consequences of C19 vaccines. A current instance is his meticulously referenced 12 Sep 2022 follow-up letter, Sen. Johnson to CDC Director Walensky: You Have Failed to Provide Data on COVID-19 Vaccine Adverse Events wherein he writes, “You have failed to explain why the CDC made inconsistent statements about the data it generates to track these adverse events. Moreover, even though I clearly asked CDC to provide the data that it supposedly generated to track vaccine adverse events, you failed to do so.” A follow-on to confronting CDC lack of transparency is a 3 Oct 2022 report by Zachary Stieber in The Epoch Times on Newly Obtained Emails Shed More Light on CDC’s False Vaccine Safety Monitoring Statements.
The profound derogation of public trust in the Federal Government agencies responsible for protecting and promoting the health of everyone in the US—including the FDA, CDC, NIH, NIAID, and all Departments within HHS—cannot be overstated. Across the Atlantic, a September 2020 data leak from the European Medicines Agency (EMA, the equivalent of the FDA), revealed how mRNA integrity in the Pfizer vaccine had serious quality control issues ranging from 78% down to 55%. Steve Kirsch wrote about this on 31 August:
Citing the work of another Substack author and a video produced in 2020,
The video is just 14 minutes long and is very well done. The findings are all consistent with what I and others have long suspected: the vials are all different. The key finding is the reason they won’t let anyone analyze the vials: mRNA is not intact. The BMJ wrote about this on March 10, 2021 [my comments are in brackets]...
Integrity of mRNA is supposedly what FDA regulates and verifies. Jennifer Margulis and Joe Wang presented their analysis of how Pfizer COVID Vaccine Safety Varies from Lot to Lot (Bioregulatory Medicine Institute, 31 Aug 2022). (Margulis has an impressive lineage: her mother was one of the most important microbiologists of the 20th century, her father was an X-ray crystallographer, her uncle won a Nobel Prize in Physics, and her other uncle, former chair of the Math Department at MIT, is known for having solved several “unsolvable” math problems.)
Some final indicators of what we are dealing with regarding C19 vaccine consequences are the following sources. Initially launched in December 2021, How Bad Is My Batch? catalogs and lists “Batch codes and associated deaths, disabilities and illnesses for C19 19 Vaccines.” Consequences of these varying batches of C19 shots being injected into people include this partial list of sources bearing witness to people suffering injuries as well as deaths from the C19 shots. On 3 Oct 2022 it was revealed by Zachary Stieber writing in The Epoch Times, that Hundreds of Thousands of Americans Sought Medical Care After COVID-19 Vaccination: CDC Data. Steve Kirsch wrote about this on 5 October in Why did the CDC hide the v-safe data from the American people for almost 2 years?
Concerning the CDC’s V-safe program, Kirsch included two snapshots of what the data showed:

The Informed Consent Action Network’s (ICAN) legal team sued the CDC twice leading to a court order requiring the release of the data. Important notes: (1) These data are limited to around 10 million v-safe users. (2) These data are limited to only pre-populated fields checked by v-safe users (for example, selecting from a list of pre-populated symptoms). (3) The information captured in free-form fields has not yet been produced and ICAN is still litigating to obtain that information. The V-Safe Data is available for download from ICAN.
The above only begins to scratch the surface of the damage to countless people’s lives caused by the clear and unquestionable evil of these C19 shots. They are NOT safe, and NOT effective. Mathew Crawford is a prime mover in the creation and operation of the CAMPFIRE WIKI nexus. See Appendix 3, The Vaccine Wars for a chronological listing of his analysis of the C19 shots. For small lists of analyses of and reporting on C19 vaccine deaths see Appendix 4 and for C19 vaccine injuries see Appendix 5.

|
“
|
For me what’s really important about ivermectin is that ivermectin is actually the key to unlocking all the secrets of this pandemic. Because it turns out hydroxychloroquine was squashed as well, and if ivermectin or hydroxychloroquine had been approved, there would have been no lockdowns, there would have been no masking or any of that necessary because they’re really good at reducing transmission. Ivermectin especially [as] it works for prevention as well as treatment. There would have been no Emergency Use Authorization of experimental novel treatments and that includes the new gene-based vaccines. If you want to understand what Covid is all about then you've got to start with ivermectin and that really unlocks the whole mystery.
|
|
—Dr. Tess Lawrie, Former WHO Consultant Exposes Takedown of Ivermectin, The Highwire, 3 Mar 2022
|
|
From the Spring of 2020 on, official pronouncements uniformly asserted that the SARS-CoV-2 virus was novel and the only way to counteract it was through development of a new vaccine. On 31 January 2020 HHS Secretary Alex Azar declared a Public Health Emergency. On 4 February 2020 Mr. Azar determined FDA was now justified in enacting an Emergency Use Authorization (EUA) wherein “the FDA Commissioner may allow medical countermeasures to be used in an emergency to diagnose, treat, or prevent serious or life-threatening diseases or conditions caused by such agents, when there are no adequate, approved and available alternatives.” [emphasis added]
Mr. Azar also invoked the 2005 Public Readiness and Emergency Preparedness Act (PREP Act), effective 4 February 2020 which, “provides liability immunity related to the manufacture, testing, development, distribution, administration and use of medical countermeasures against chemical, biological, radiological and nuclear agents of terrorism, epidemics, and pandemics”. The legal immunity protection lasts until 2024.
The groundwork was now laid to make waiting for a new vaccine the only “solution” to the “novel” virus while simultaneously shielding pharmaceutical corporations from any injury or death resulting from the experimental shots. From this Catch-22 witch’s brew, was spawned the unconscionable program to marginalize, dismiss, censor, perform character assassination, suspend and revoke medical licenses, and worse for medical practitioners seeking to see to the needs of their patients, especially in the US and Europe.
One year ago I wrote about Early Treatment Remedies Available in 2020 to treat Covid-19. Everything covered then is that much more critically and tragically relevant today. One full year later, the choke-hold drive to muzzle MDs who still put their patient’s needs above the dictates of soul-less state power, continues to destroy countless livelihoods and lives. The only way for the EUA to be valid was and is if there are no adequate, approved, and available alternatives. The prior-to-2020 unthinkable consequences of this official straightjacket has prevented Medical Doctors from fulfilling their Hippocratic Oaths to First Do No Harm. Increasingly baseless, concerted attacks mounted in corporate state media and by government officials and academic “experts” have targeted Doctors employing their intelligence, training, experience, and knowledge to find efficacious remedies for their patients suffering effects of the SARS-CoV-2 virus.
This government-imposed straightjacket is the justification FDA brandishes to deny approval of Chloroquine, Hydroxychloroquine, Ivermectin, Budesonide, Vitamin D, and a host of other effective, safe, and cheap remedies for C19 early treatments. See Appendix 6 for the current readout of COVID-19 early treatment: real-time analysis of 2,175 studies.
In the past 12 months, the saga has continued of physicians around the world applying their expertize to lessen suffering from the effects of SARS-CoV-2. So much was already understood in 2020. Witness the understanding amassed by November of that year:Beginning in March of 2020, all the assertions by the likes of Tony Fauci et al about how, We don’t know what to do except to create a never-been-tried-before-for-a-coronavirus vaccine and get it into everybody and Go home if you get sick, isolate yourself, and if it really gets bad go to the hospital. But the reality was and is, We DO KNOW WHAT TO DO about this virus. As an example, looking back to 2020, Dr. Peter McCullough wrote on 12 Oct 2022 in McCullough Protocol©: Three Phases of Index COVID-19:
When McCullough et al, described three overlapping phases of COVID-19 illness in the “index” or first occurrence (viral replication, cytokine storm, and thrombosis) it allowed clinicians to approach the illness in a sequential manner and led to the understanding that a single drug would not provide comprehensive treatment for those at the highest risk of requiring hospitalization....

It is disappointing that none of the Infectious Disease Society of America (IDSA) or National Institutes of Health Guidelines (NIH) properly conceptualized the illness in this manner. As a result, the first NIH guideline in October of 2020, indicated that no treatment should be given to a patient in the ambulatory phase and only when hospitalized and requiring oxygen should the antiviral remdesivir be given as the initial therapy. For the average patient who has been ill at home for two weeks, one can see from the figure that the viral proliferation phase is nearly complete, and the patient is well into cytokine storm (inflammation) and pulmonary microthrombosis causing oxygen desaturation and respiratory distress....The above cites the reference:
Correct understanding of the multifaceted and phased natural history of COVID-19 led to the innovation of multi-drug therapy that begins ideally on day one of the illness and with the goal of shutting off the progression of disease to avoid hospitalization, mechanical ventilation, and death. When the debacle of government agency pandemic response is reviewed, likely this figure to appear and watch agency officials answer questions on why the US featured the late use of remdesivir for inpatient treatment? Expect questions on why the agencies proposed the antiviral Paxlovid to work as monotherapy? Finally, there will be strong statements about how our government agencies failed to ask for “second opinions” from experts who were gaining insight on the phases of COVID-19 and matching successful therapy for patients in the community using multidrug regimens.
Tess Lawrie, MD, PhD, has been called The Conscience of Medicine. As the Director of The Evidence-based Medicine Consultancy Ltd, Dr. Lawrie has worked as an independent external research consultant to organizations such as the World Health Organization. She is a co-founder, and on the Steering Committee, of the World Council for Health, a non-profit initiative for the people, that is informed and funded by the people. A global coalition with 170+ partner organizations, 40+ Countries with WCH partners, and 10+ Committees and workgroups, the WCH’s health-focused initiative and civil society groups work to broaden public health knowledge and sense-making through science and shared wisdom.
In a cogent May 2021 presentation about Why Are We Not Using Ivermectin For Covid? Dr. Lawrie concluded her analysis with the following:
The authorities are ignoring the facts. Why aren’t we using ivermectin? Ask yourself who would have lost out if people had had access to effective generic medicines in March last year? As doctors and scientists, we currently find ourself at a peculiar place in medical history where rigorous scientific evidence, doctor’s expertise and experience, the foundations of our practice have been undermined by a relentless onslaught of disinformation. Why won’t the world’s health authorities and developed country governments approve ivermectin for Covid? I’ll leave it up to you to figure out. But if I could offer one piece of advice from my heart to yours, please take responsibility for your health. Stop outsourcing it.
In our present scoundrel time, Tess Lawrie echoes Ivan Illich’s perception that cultural iatrogenesis restricts the vital autonomy of people by undermining their competence in growing up, caring for each other, and aging. Ivermectin was—and still is— on the WHO’s list of Essential Medicines. It is a drug that previously has been taken by 250 million people every year as well as being a [2015] Nobel prize winning medicine due to its increasing usefulness across a range of different illnesses. For analysis of the remarkable antidotes repurposed drugs including hydroxychloroquine and ivermection provided to address illness caused by the SARS-CoV-2 virus as well as the directed information black-out and suppression of same, see the 18+ months examination in Appendix 7 of Mathew Crawford’s, The Chloroquine Wars.
Dr Lawrie’s statement above, that ivermectin is the key that unlocks all the secrets of the so-called pandemic, is writ large in her crushed hopes of seeing this medication approved for people suffering the effects of the SARS-CoV-2 virus. The nail in the coffin that buried ivermectin is the horrific account of how Dr. Andrew Hill, tasked to report to the WHO on dozens of global studies evaluating ivermectin to treat C19, published his findings in January 2021 that killed the hopes for rapid approval of ivermectin. (See also: “The Moral Disintegration of Andrew Hill: After playing a critical role in preventing patient access to Ivermectin, Andrew Hill authored a paper advocating for expanded access to Paxlovid - This brazenly hypocritical stance illustrates how Pharma is able to exploit human nature to manipulate people into rationalizing away their moral convictions and guilty conscience”, Ashmedai, Resisting the Intellectual Illiteratti, 9 Oct 2022)
In A Letter to Andrew Hill from Dr Tess Lawrie (7 Mar 2022, 18:53), she states how “There was much at stake in January 2021 when you put your paper on Research Square, both in human lives and in profits.” A year-plus after the burial of ivermectin, Dr. Lawrie implored Dr. Hill to name the people who caused him to change his conclusions:
Together you and I could have saved millions of lives and so much suffering. Look what they're doing now, Andy. They're injecting our children with experimental vaccines. If only you had made a different choice and if only I could have persuaded you to do the right thing. I ask you now to make that difficult choice, to do what is in the best interest of your friends and countrymen, and to do what is in the best interests of humanity at large. Help to expose the corruption of science by coming forward to explain the pressure you have been under to undermine the evidence on ivermectin. Explain the delicate situation you were in January 2021 and name the people who influenced you to change your conclusions. Only then can we start to fix the harm that's been done. We will forgive you Andy, but come forward.
Appendix 8 includes noteworthy books illuminating successful treatment by physicians exercising their intelligence and wisdom with clarity and coherence of illness caused by the SARS-CoV-2 virus. If these accounts were reported in print, broadcast, and digital media, there would be no epidemic of C19.

In concert with demonstrating ivermectin’s benefits, Dr. Kory catalogs here the indefensible Disinformation war on ivermectin: Timeline of Major Battles In the Global War on Ivermectin
The effectiveness of following early treatment protocols to enable recovery from C19 cannot be overstated. As Dr. Fareed wrote on 10 Dec 2020—reported in, Dr. George Fareed and Dr. Brian Tyson Early Treatment Protocol (2022) (OneDayMD, 15 Sep 2022)—“The earlier the treatment can be started after the start of the infection, the better and more rapid the recovery (as well as the reduction in the risk of spread/contagious period). This would mean that the patient should optimally start the treatment in the first 4 days of the infection and within five days of exposure. It usually is based on symptoms which start within 1-4 days of viral entry into the upper respiratory system. Even starting the multi-faceted treatment later (7-10 days after infection) is also very worthwhile if severe pneumonia necessitating hospitalization has not yet set in.”
Mathew Crawford wrote Chapter 8: Our Statistical Research Summary in Overcoming the Darkness - How Two Doctors Successfully Treated 7000 Patients. He reproduced the following from Chapter 8 in his Rounding The Earth Newsletter on 13 January 2022: Low Rates of Hospitalization and Death in 4,376 COVID-19 Patients Given Early Ambulatory Medical and Supportive Care. A Case Series and Observational Study. The following is from a segment further along in Chapter 8. It is reproduced here with the express permission of Dr. George C. Fareed.
I find repetition and consistency of scientific results to be most persuasive. Both in my work with Dr. Tyson and Dr. Fareed, and elsewhere, I have found astonishing consistency in the efficacy of early treatment—particularly from the use of hydroxychloroquine and ivermectin—to combat COVID-19.
- Dr. Tyson and Dr. Fareed: approximately 7,000 patients with four hospitalizations and zero deaths.
- Dr. Raoult: He and his colleagues have published scores of papers,[endnote 90: Mediterraneev Infection. (April 14, 2020), “PUBLICATIONS & PREPRINT IHU.” Retrieved December 7, 2021, from https://www.mediterranee-infection.com/pre-prints-ihu/.] some of which I have read, but as best I can recall one summarized the use of hydroxychloroquine early treatment protocols applied to approximately 8,000 patients, with just five deaths, as of sometime in 2021.
- Dr. Ben Marble: Dr. Marble is the first physician to treat patients in all fifty states. He and his staff have treated 65,000 patients at the early stages of COVID-19 with what he describes as a 99.99% survival rate, meaning in the ballpark of six or seven total deaths.
- Dr. Vipul Shah: As of June 2021, Dr. Shah had lost just five out of around 8,000 patients using hydroxychloroquine during the first pandemic wave in India, then ivermectin during the second. He explained to me that he switched treatment protocols due to Facebook’s censoring of his communication with other physicians and patients.
- Dr. Vladimir Zelenko: Out of around 3,000 patients, only two died.
- Dr. Brian Procter: Through September 2020, Dr. Procter put 922 patients through his treatment protocol with six hospitalizations and one death.[endnote 91: Procter, Brian C et al. “Clinical outcomes after early ambulatory multidrug therapy for high-risk SARS-CoV-2 (COVID-19) infection.” Reviews in cardiovascular medicine vol. 21,4(2020): 611-614. Doi:10.31083/j.rcm.2020.04.260.] I lost track of his tally after Twitter revoked his account.
- Dr. Luigi Cavanna: By April 2020, Dr. Cavanna stated in an interview with Time that he had treated 280 outpatients in COVID-ravaged Italy with around 5% hospitalization and zero deaths.[endnote 92: Berardi, F. (April 9,2020). “The Italian Doctor Flattening the Curve by Treating COVID-19 Patients in Their Homes.” Time. Retrieved December 7,2021, from https://time.com/collection/coronavirus-heroes/5816874/italy-coronavirus-patients-treating-home/.] inpatients after word of his success spread.
- Senior Clinical Pharmacist Abdulrahman Mohana: In a study of 238 outpatient fever clinics prescribing hydroxychloroquine to 2,733 COVID-19 patients in Saudi Arabia, there were no ICU admissions or deaths reported.[endnote 93: Mohana, Abdulrhman et al. “Hydroxychloroquine Safety Outcome within Approved Therapeutic Protocol for COVID-19 Outpatients in Saudi Arabia.” International journal of infectious diseases: IJID: official publication of the International Society for Infectious Diseases vol. 102 (2021): 110-114. doi:10.1016/j.ijid.2020.10.031.]
- Dr. Heather Gessling: By September 2021, Columbia, Missouri’s top- ranked family physician had treated around 1,500 patients, losing just one due to nonadherence to treatment. She was later fired as Chief of Staff from the hospital where she worked.
- Dr. John Littell: Well over 2,000 patients were treated early with around ten deaths (all Delta variant infections).
- Dr. Mollie James: Around 1,000 patients were treated, five hospitalizations (all relatively late to treatment among the early treatment patients), and zero deaths.
- Dr. Ryan Cole: Around 350 patients with zero hospitalizations and zero deaths.
- Dr. Pierre Kory: Between 150 and 200 patients with one hospitalization and zero deaths.
- Dr. Kimberly Milhoan: Around 200 were treated with a few hospitalizations and zero deaths.
- Dr. Katarina Lindley: Around 100 were treated with five hospitalizations and zero deaths.
- Dr. Deborah Chisholm: Around 100 were treated with zero deaths.
What I see in these results is repetition. And consistency. The 100,000 or so patients represented here suffered around thirty total deaths, which comes out to a 99.97% survival rate. Most of these patients were in the U.S., and the aggregate fatality rate among these patients is around 98% lower than the U.S. average, just as I had observed when aggregating global data more than a year ago. Note that the treatments prescribed among these physicians vary with some patients receiving hydroxychloroquine, some receiving ivermectin, and some receiving both medications.
Most of these doctors put on their Captain Obvious hats and give their patients vitamins and zinc, too. They prescribe corticosteroids or monoclonal antibodies where they see fit. They practice empiric medicine, using practiced judgments to fit the treatment to the patient and the symptoms present. The whole is never really the sum of the parts, so it is impossible, not to say inappropriate, to ascribe a certain proportion of this dramatic success to any one medicine, and while individual studies can sometimes confirm their success, no study of any of the treatments in isolation can logically confirm their failure in combination with the rest.
These are not the only doctors whose stories I could tell. I’ve communicated with several others, and heard secondhand anecdotes about many more. I do not have statistics to report for all of them. Within the numbers that I do have, the collective mortality rate is not much different from background mortality (people who would have died under normal circumstances), and while I do not know the full details, a substantial portion of the mortality is reportedly associated with nonadherence to the prescribed treatments.
Repetition. Consistency.
I have yet to talk to or even hear about a doctor who stopped providing early ambulatory treatment of COVID-19 patients after failing to keep nearly all of their patients healthy. Not one. Not from anywhere in the world after communicating with hundreds of researchers and physicians, discovering that tens or hundreds of thousands of physicians around the globe have used these early treatment medications and principles during the pandemic. Either these treatments work, or they’re all physicians with previously unimpeachable careers who independently decided to lie to cover up their delusions, and without one whistleblower or shred of evidence contradicting their stories.
What else could I conclude?
Repetition. Consistency.
Dr. Fareed’s devotion to serving patients’ needs and his fearless adherence to the Hippocratic Oath is a stellar beacon for the sacredness of the healing arts. See an hour-plus of his Patient Testimonies (produced 22 Jun 2022) and a 23-minute interview with Dr. Fareed in early July 2022 from Iguaçu Fall, Brazil, upon the conclusion of the 2nd World Congress of the World Council for Health and Doctors for Life Conference on Doctor Helps Successfully Treat Over 12,000 Covid Patients -Dr. George Fareed, MD.
There are a number of highly effective and proven treatment protocols to prevent and treat COVID:
|
“
|
Without freedom, everything we regard as quintessentially valuable in human life will be lost. Physical death is a blessing to a human being who has been enslaved to the point where all but the most basic needs of survival are met. These past three years, consumed as they have been by all things Covid, have laid bare the best and worst of us, and have thrown into starkest relief the crux upon which our battle for the future rests.
|
|
—Emanuel E. Garcia, The Anatomy and Psychology of Power, 2 Nov 2022
|
|
With all the above amassed knowledge and ensuing treatment protocols that have been established with proven efficacy, it beggars understanding of why state sanctioned witch hunts are going after physicians who advise truly safe, effective, and cheap alternatives to the one-size fits all experimental injections being universally pushed by government “health officials,” bureaucrats, and academic talking heads.

The recent passage of California Assembly Bill 2098 is the first-of-its-kind overt legal bid by the state to punish doctors—including suspension of their medical licenses—for spreading “misinformation” or “disinformation“ about C19 with their patients. The statute defines misinformation as “false information that is contradicted by contemporary scientific consensus contrary to the standard of care,” and disinformation as “misinformation that is deliberately disseminated with malicious intent or an intent to mislead.”
Reiterating analysis from October 2021 concerning the actual definition of “disinformation” (emphasis added):
Retired health sciences librarian Elizabeth Woodworth’s critical analysis, “COVID-19 and the Shadowy ‘Trusted News Initiative’, How it Methodically Censors Top World Public Health Experts Using an Early Warning System” illustrates the war-is-peace, black-is-white, slavery-is-freedom inverted reality humanity is being subjected to and oppressed by. Among many cogent observations Woodworth articulates, what disinformation actually means is especially relevant here:This question has been sloppily handled by the mainstream media, which often confuses “misinformation” (unintentionally misleading information) with what they mean, “disinformation,” which is deliberate. Several dictionary definitions agree on that point:
Given that these definitions specify deliberate government action, it seems odd that the TNI has identified a scattered online public as the source of intentional false information and propaganda – especially concerning elections and health policy.
- American Heritage: “Deliberately misleading information announced publicly or leaked by a government or especially by an intelligence agency in order to influence public opinion or the government in another nation.”
- Merriam-Webster: “False information deliberately and often covertly spread (as by the planting of rumors) in order to influence public opinion or obscure the truth.”
- The OED (Oxford English Dictionary): “The dissemination of deliberately false information, esp. when supplied by a government or its agent to a foreign power or to the media, with the intention of influencing the policies or opinions of those who receive it.”

Physicians are speaking out against this advancing medical totalitarianism. Primary care physician Jeff Barke, MD, and psychiatrist Mark McDonald, MD, have filed a federal lawsuit against the Medical Board of California and state Attorney General Rob Bonta declaring AB 2098 unconstitutional and seeking a preliminary injunction to prevent it from being enforced.
The private power behind this agenda to censure physicians who do not parrot the official narrative of vaccines uber alles and strip them of their livelihoods is the little-known Federation of State Medical Boards, a tax-exempt 501(c)(6) charity. Founded in 1912, it is older than the US Department of Health and Human Services (renamed in 1978; formerly Dept of Health, Education, and Welfare, created in 1953; formerly Federal Security Agency created in 1939) and all its subagencies including FDA, NIH, CDC, and CMS. While the Federation of State Medical Boards (FSMB)—and its global arm, the International Association of Medical Regulatory Authorities (IAMRA)—are virtually unknown by medical doctors as well as the general public, their influence and power is far reaching. As private charities, both organizations are funded by anonymous donors who oversee the disciplinary action of licensed medical doctors.
Paul Martin Kempen, MD, PhD, is a past President of the Association of American Physicians and Surgeons. In 2016 he wrote in the Journal of American Physicians and Surgeons about The Influence of the Federation of State Medical Boards (FSMB) on State Medical Boards:
Despite the implications of its name, the Federation of State Medical Boards, Inc. (FSMB), like the American Board of Medical Specialties (ABMS) and its 24 affiliates, is not a governmental authority. None of these entities have official legislative or regulatory power afforded by any federal or state government.[1] FSMB, however, uses its contacts and influence with state medical boards (SMBs) to advance its corporate products. This may be called “crony capitalism.” When founded decades ago with the support of the American Medical Association, when licensing and medical regulation were in their infancy, these organizations collaborated closely, serving a purpose in creating standards for students and trainees entering the profession. However, FSMB has now become part of a lucrative industry that imposes significant expense without value onto patients and practicing physicians, expanding their markets by making demands upon their “return customers”: licensed physicians. FSMB is tax exempt under section 501(c)(6) of the Internal Revenue Code, although it is in the business of selling to physicians “products and services” that become “needed” only after it lobbies government agencies, such as SMBs, to require them through legislation, organizational demand, and administrative policy. This is known as regulatory capture of a market.[1] [2] [3] These methods have caused FSMB to become a corporate juggernaut with gross receipts of $50 million per year. It is now a premier “physician adverse” organization.[4]
Six years ago, the FSMB collected “gross receipts of $50 million” In 2021 the FSMB spent $280,000 lobbying the federal government; for the first six months of 2022, it spent $160,000. According to FSMB Inc Audit for the period ending Apr 2021,
Dr. Emanuel Garcia is a Philadelphia-born psychoanalyst and psychiatrist who emigrated to New Zealand in 2006. In Subverting Medicine: The Role of the Federation of State Medical Boards he wrote about how the FSMB and the IAMRA “share the very same address near Dallas: 400 Fuller Wiser Road, Euless, TX 70039.”
Coincidence?
The Chair-Elect of the IAMRA, Joan Simeon, just happens to be the CEO of the Medical Council of New Zealand, and the Secretary of the IAMRA, Dr. Humayun Chaudhry, just happens to be the President and CEO of the FSMB. The Medical Councils of Ireland and New Zealand are members of the IAMRA....
The outstanding question remains: Where does the FSMB derive its authority to regulate United States medical boards and, through its apparent international partner, the IAMRA, direct medical councils around the world to discipline doctors?
In concert with the outstanding question posed above is the fact that as private charities, both organizations are funded by anonymous donors. What industry besides pharmaceutical corporations have as much to gain by making anonymous, off-the-books donations to the FSMB and IAMRA? In 2021 Dr. Kempen wrote about the critical necessity of understanding the bureaucracy of the medical certification industry as well as the development and very nature of certification in The Curse and Corporate Cult of Certification in America.
Physicians are abandoning leadership in medicine by subordinating their professional integrity to non-physicians and administrators. Unless physicians start taking back medicine with leadership, we will see only continuing decline and subjugation of professionalism to non-physician “providers,” government, insurance, and corporate dictates... The certification industry is antiquated, like slavery, leeches, and bloodletting. Medical costs are now excessive, and antiquated concepts must be addressed, including needless certifications, and especially recertifications [Maintenance of Certification®].... In the profession of medicine, physicians are not the governed, but are sovereign. Practice must be subject only to the welfare and needs of the patient. We must together secure our profession for the public welfare against any corporate, legislative, or material intrusions.... The job remains for each individual to refuse to be indoctrinated and extorted by the ever-growing certification industry. Our profession itself is under attack from multiple sides. Freedom is not free! If you do not resist, you are part of the problem. Change bylaws. Sue for your rights. Physicians are in demand and must fight the demise of professional patient care actively, including the use of ever more numbers of poorly trained non-physician “providers” who are compliant only with “algorithm medicine.”
When one searches on “Association of American Physicians and Surgeons” the second result is the Wikipedia page which states in its opening paragraph that the AAPS “is a politically conservative non-profit association that promotes conspiracy theories and medical misinformation”. Wikipedia co-founder Jimmy Wales is quoted on the About page, “Imagine a world in which every single person on the planet is given free access to the sum of all human knowledge. That's what we're doing.” Mr. Wales is on the advisory board of NewsGuard, “The Internet Trust Tool”. NewsGuard, the Trusted News Initiative, and the Covid Collaborative stand out as paid-for-hire Arbiters of Reality whose business is managing perceptions for its corporate state empire directors.
Wikipedia’s editorial framework and its claim of providing “free access to the sum of all human knowledge” is classic Orwellian Newspeak, subterfuge imbued with propagandistic language embodying the very best Crimestop has to offer.During the past 19 years Wikipedia has risen to the admirable status as the world’s most formidable and trusted encyclopedia to educate and inform the public about acceptable and unacceptable medical systems, therapies and interventions. Although there are no accurate figures, there have certainly been billions of searches on Wikipedia about health topics over the years. However, there is a problem. And it is a very serious and potentially life-threatening problem about relying upon Wikipedia’s content regarding many medical modalities. For example, virtually everything that comes up for searches on Alternative and Complementary Medicine (CAM) is negative and provides an unscientifically founded and derogatory narrative.
Dr. Colleen Huber is a Naturopathic Medical Doctor and an author. She covers a wide swath about corruption of the healing arts, including the FSMB, in “Meet the Tyrants Who Corrupted Your Doctor - Since the red dawn of COVID, both my patients and Substack readers have expressed dismay over how idiotic doctors seemed to have become. Here’s how it happened and who was involved.”
Enormous windfalls of money came to US hospitals through the US Cares Act in early 2020, to basically finance the extravaganza theatrical production of a pandemic, when in fact, from an epidemiological viewpoint, we were dealing with a fairly typical annual flu season: 0.15% infection fatality rate for COVID, when all was said and done, but 0.17% for flu in 2006 to 2008. What was the purpose of the destructiveness toward our lives and livelihoods, our kids’ education, our respiratory pathways, our bodily autonomy, our small businesses, and ultimately our trust in medical and governmental leaders? It may be that the most sinister manifestations of the COVID era are only beginning to unfold.So doctors are now employed by hospitals that received millions, even hundreds of millions, for adopting the most anti-Hippocratic treatments possible for COVID: over-pressurized ventilators blowing out healthy lung tissue, the death-row drugs midazolam and morphine given in multiple times the known deadly dose, in synergistic lethal combination, the kidney-killing drug Remdesivir, and the withholding of the obviously benign and even Nobel Prize-winning drug ivermectin....
But there is an additional stranglehold on doctors beside their new institutional employers.
That is the nearly unknown Federation of State Medical Boards, which I discuss here, and which came to my attention via a recent lawsuit, by a doctor who is sticking to his principles. Dr. Paul Thomas, pediatrician, is suing the Oregon Medical Board for $35 million. The grounds: After Dr. Thomas published the health outcomes of vaccinated vs unvaccinated children, five days later, the Oregon Medical Board seized his license. Dr. Thomas has cited undisputed data in his criticism of the intense US vaccination schedule imposed on children, and the harms they’ve suffered as a result.
As a private entity, the Federation has zero legal or statutory authority to dictate anything to anyone, either conferred by the US Constitution, the Congress or any state legislature. Yet it has set itself up as the tribunal for judgment and “discipline” to use their unlawful word, against state medical boards that do not conform to the letter of the Federation’s desires, according to Article 12 of their bylaws. Then, in the confession below, one can see their pressure to threaten the licenses of doctors.
... The sooner and more decisively the private sector is stopped from violating the free speech rights of the citizenry – including healthcare professionals’ rights to express their thoughts freely on medicine and other topics, without fear of retaliation – the sooner we can return to a system of medicine that actually places patient wellbeing, fully informed consent and best interests in first place, as highest priority. And the sooner medicine can return to its oath: First Do No Harm.
In 1974 Ivan Illich warned that, “Our increasing confrontation with medical nemesis now lends new significance to the alternative: either society must choose the same stringent limits on the kind of goods produced within which all its members may find a guarantee for equal freedom, or society must accept unprecedented hierarchical controls.” Fast-forward forty-eight years and see clearly now our war with medical nemesis demands we face and respond to what Illich observed:
The technical and the nontechnical consequences of institutional medicine coalesce and generate a new kind of suffering: anesthetized, impotent, and solitary survival in a world turned into a hospital ward. Medical nemesis is the experience of people who are largely deprived of any autonomous ability to cope with nature, neighbors, and dreams, and who are technically maintained within environmental, social, and symbolic systems. Medical nemesis cannot be measured, but its experience can be shared. The intensity with which it is experienced will depend on the independence, vitality, and relatedness of each individual.... Medical nemesis is resistant to medical remedies. It can be reversed only through a recovery of the will to self-care among the laity, and through the legal, political, and institutional recognition of the right to care, which imposes limits upon the professional monopoly of physicians.
|
“
|
US Government since 1969 has incrementally transferred/hidden the joint DOD+HHS Chemical and Biological Warfare Program (50 USC 32) in the Public Health Service Act (42 USC 201) and Food Drug and Cosmetics Act (21 USC 9), such that federally-funded, federally-directed public health programs and products are actually bioterrorism programs and biological and chemical weapon attacks.
|
|
—Katherine Watt, Memo re: US federal law on bioweapons reclassified as public health measures. Bailiwick News, 21 Nov 2022
|
|
Gain-of-Function Research is defined on the US HHS site as, “research that improves the ability of a pathogen to cause disease, help define the fundamental nature of human-pathogen interactions, thereby enabling assessment of the pandemic potential of emerging infectious agents, informing public health and preparedness efforts, and furthering medical countermeasure development.” [emphasis added] In Dr. Peter McCullough’s words, “the true objective of gain of function research [is] to develop new, commercially valuable vaccines against the very pathogens that the Dr. Frankensteins are creating.”
Dr. Byram W. Bridle is Associate Professor of Viral Immunology in the Dept of Pathobiology at the University of Guelph. On 18 Oct 2022, Dr. Bridle posted his assessment of “Lab in Boston Made What Could Be A Super-Killer SARS-COV-2 - Extreme Danger: This is Gain-of-Function Research on Steroids”. In his analysis of the pre-print article, “Role of spike in the pathogenic and antigenic behavior of SARS-CoV-2 BA.1 Omicron”, he pointed out how gain-of-function research did result in the SARS-CoV-2 virus:
Apparently, [the authors] were trying to figure out what role the spike protein has played in the ability of the Omicron variant to escape the far-from-sterilizing COVID-19 jab-induced immune responses, as well as its role in pathogenicity (how the virus causes disease). Here it is in the authors’ words:“We generated chimeric recombinant SARS-CoV-2 encoding the S gene of Omicron in the backbone of an ancestral SARS-CoV-2 isolate and compared this virus with the naturally circulating Omicron variant.”I don’t care what the hypothesis of the study was. The results are nightmarish.
To the Point: A Potentially Deadly SARS-CoV-2 was Engineered
When the chimeric SARS-CoV-2 was tested in mice that express the same high-affinity viral entry receptor that people do, the authors dropped this bombshell...
“...while Omicron causes mild, non-fatal infection, the Omicron S-carrying virus inflicts severe disease with a mortality rate of 80%.”This is a classic example of gain-of-function research.
It was gain-of-function research that resulted in SARS-CoV-2 in the first place. People like U.S. senator and physician Rand Paul have essentially proved this fact. Notably, while squirming under Senator Paul’s questioning, Anthony Fauci repeatedly denied ever funding gain-of-function research, let alone with respect to SARS-CoV-2. With this in mind, note one of the key sources of funding for this current research that has generated a super-deadly SARS-CoV-2; as disclosed by the authors...
“National Institutes of Health, NIAID grants R01 AI159945 (to SB and MS) and R37 AI087846 (to MUG)”NIAID is the National Institute of Allergy and Infectious Diseases, of which Anthony Fauci is the director! I am keen to see if Fauci will still declare under oath that his agency has never funded gain-of-function research related to SARS-CoV-2.
The paper trail of US government funding for gain-of-function research is an indisputable indicator of federal agencies’ direction and involvement in the practice of improving the ability of a pathogen to cause disease. More on this below. Dr. Bridle goes on to outline additional gain-of-function issues concerning the recklessness and dangers of what are, in fact, US violations of the Biological Weapons Convention Treaty, signed and ratified by the United States. It is a violation of the BWC Treaty to develop, acquire, retain, or produce any biological agent not justified for prevention or peaceful purposes.

Further, United States Federal Code 12 U.S.C. Chapter 10 § 175 expressly prohibits such biological weapons, the creation of which is a criminal offense. Dr. Bridle continues,
It Gets Worse: Providing a Recipe for a Super-Pathogen
A good scientific paper should be written in such a way that other scientists in the respective field(s) of expertise could repeat the experiments to determine whether or not the results can be replicated. I am a viral immunologist and I reviewed the materials and methods section. I am confident that my research team could use this information to make the same chimeric virus. My team would never do this. However, I cannot speak to the morality of potential bioterrorists who could just as easily replicate the work should they have access to basic laboratory facilities.
In essence, the 23 authors of this paper have provided a recipe for a potentially potent bioterrorism agent. It is in the public domain and can no longer be eliminated from cyberspace.
Remarkably, It Gets Even Worse
The naturally occurring SARS-CoV-2 is what is known as a ‘containment level-3 (CL-3) pathogen’ (Americans would call it a ‘biological safety level-3 pathogen’). This means that research with this virus must be conducted in a CL-3 facility. Such facilities have sufficient biosecurity to keep a CL-3 pathogen contained. A major potential problem with gain-of-function research is that it can amplify the danger and/or infectivity of a pathogen. This is exactly what happened in the current case.
In short, the research project started with a non-lethal SARS-CoV-2. What emerged is a virus with the potential to be much more dangerous. This means that the 23 authors of the article may have ended up with a CL-4 pathogen housed in a CL-3 facility. The latter type of facility is not designed to contain a CL-4 pathogen.
This is an excerpt from the materials and methods section of the paper...
“All procedures were performed in a biosafety level 3 (BSL3) facility at the National Emerging Infectious Diseases Laboratories of the Boston University”Here is how the United States Centers for Disease Control describe pathogens that must only be handled within CL-4 facilities...“The microbes in a BSL-4 lab are dangerous and exotic, posing a high risk of aerosol-transmitted infections. Infections caused by these microbes are frequently fatal and without treatment or vaccines. Two examples of microbes worked with in a BSL-4 laboratory include Ebola and Marburg viruses.”
- Can SARS-CoV-2 be transmitted via aerosols? Yes
- Is the chimeric SARS-CoV-2 frequently fatal? Yes, in mice; unknown in humans
- Do effective treatments exist? The most effective ones have been outlawed
- Do effective vaccines exist? No. Laughable vaccine-wannabes exist, though.
So, should the chimeric SARS-CoV-2 have only been handled in a CL-4 facility. Likely yes, but, “All procedures were performed in a biosafety level 3 facility”.
If this virus were to get released into the public, it could result in a global catastrophe should its fatality rate, which is similar to ancestral SARS-CoV-2 be coupled with the much higher transmissibility of Omicron. Although this virus was not evaluated in humans, pre-clinical studies are used to try to predict what would happen in people. There is the theoretical potential for the virus to be less or equally deadly in people as compared to mice. However, for all we know, the virus could be even more deadly in people than it was in mice. The original SARS-CoV-2 did not prove to be particularly deadly in people, but it did not have anywhere near the transmission potential of the Omicron variant.
Dr. Jessica Rose[1][2][3] is a viral immunologist and computational biologist. On 18 October, she too posted an evaluation of the above pre-print, acknowledging Dr. Bridle’s assessment that correctly points out, “they basically created and published a recipe for a deadly pathogen (80% mortality rate in the subjects of their experiments) of their own construction in their lab. By the way, this is precisely gain-of-function research. It couldn’t be more descriptive[:] ‘Gain-of-function research (GoF research or GoFR) is medical research that genetically alters an organism in a way that may enhance the biological functions of gene products such as transmissibility.’” Her conclusion summarizes a fundamental error and danger in pursuing gain-of-function man-made alteration of naturally occurring viruses, especially with respect to SARS-CoV-2:
[T]hey always try to justify this gain-of-function idea by saying things like: ‘we need to be able to make predictions about future pandemics’ and ‘we must pre-empt assaults on our nation’ bla bla bla. You know what? Leave it all alone! Leave the researchers alone to make beautiful discoveries that can actually benefit not only our own species, but all other species as well....SARS-nCoV-2 would fade beautifully into a memory if madmen looking for the next grant-fix would stop trying to play God. Human natural immunity does a fantastic job with controlling SARS-nCoV-2, and where it doesn’t - such as is the case in specific subsets of the human population like the elderly and frail - we have early treatment protocols. This work needs to be banned and the products of this work destroyed immediately and further gain-of-function work of this nature should be permanently banned. THIS IS NOT SCIENCE. THIS IS MADNESS.
Gain-of-function work derives from the development of biological weapons. In The United States and Biological Warfare: Secrets from the Early Cold War and Korea (1998, isbn: 9780253334725), Stephen Endicott and Edward Hagerman uncover a component of the history of the US biological weapons program wherein offensive biological weapons were deployed by the US military in Korea. The book reveals how “the US government lied to both Congress and the American public when it said that the American biological warfare program was purely defensive and for retaliation only. To the contrary, a large and sophisticated biological weapons system was developed as an offensive weapon of opportunity.” For selected excerpts from the book, see Appendix 9.
During World War II Frank Olson was recruited to the US Army Biological Warfare Laboratories at Fort—then Camp—Detrick. A biologist by profession, Olson was tasked to develop new and secret biological means for effective interrogation and warfare. Olson’s duties included experiments with aerosolized anthrax.

In August 1953, Frank Olson witnessed the killing of prisoners being held by the CIA in safe houses in Europe. The prisoners were ex-Nazis and were considered completely expendable. He witnessed the consequences of what he was working on with germ warfare. Frank Olson was murdered that November with the cover story fable that he jumped from a New York hotel window. His son Eric pursued the facts surrounding his father’s death for decades, producing the on-going work-in-progress: Frank Olson Legacy Project. Hank Albarelli spent years researching his 2009 book A Terrible Mistake - The Murder of Frank Olson and the CIA’s Secret Cold War Experiments (isbn.nu). From the Epilogue:
...I had started this project with the best of intentions to write an historical account about a perplexing mystery. Over time, due to circumstances beyond my control, that account also became a tale of tragedy and despair over the evidence of a nation that had lost its way on history’s road. It became an account of a nation whose best and brightest scientists and physicians, in their quest to preserve democracy and combat Communism, were willing to sacrifice virtually everything that was good about America, not to mention the lives and well being of innocent people. What was it that made these researchers so uncaring about the enormous amount of pain and suffering they caused? Did the physicians involved even contemplate their oaths to “first, do no harm” as practitioners of medicine? Were they no better than the Nazi doctors who had been tried and convicted at Nuremberg?
Further US development of biological warfare was starkly revealed in the October 2001 anthrax attacks occurring as the second blow of the one-two punch 11 September 2001 attacks. Graeme MacQueen’s The 2001 Anthrax Deception: The Case for a Domestic Conspiracy (2014) is THE go-to account of how “the group that carried out this crime consisted, in whole or in part, of insiders deep within the US state apparatus” and how the “anthrax attacks were meant to facilitate a seizure of power by the executive branch of government through intimidation of Congress and US civil society. They were also designed to achieve public acquiescence to and support for the redefinition of US foreign policy, replacing the Cold War with a new and aggressive global conflict framework, the Global War on Terror.”
The Global War on Terror has now been superseded by the manufactured “Global War on a Pathogen.” Twenty-plus years on, we are reaping the resulting worst consequences of intentional biological warfare. The following summarizes portions of the background of Richard Fleming, MD, PhD, JD, and his 2021 book:
Dr. Richard M. Fleming is a physicist, nuclear cardiologist, and attorney with a lifetime of research in physics, medicine & law. He is a Fellow of the American College of Physicians and a Fellow of the American Society of Internal Medicine, he is a medical patent expert, has authored hundreds of medical papers, and has sat on review boards of medical journals. He has spent decades investigating what causes multiple health problems including heart disease, cancer, and SARS-CoV-2/COVID-19. He joined the American Heart Association in 1976 and actively began teaching and researching heart disease; including both what causes heart disease and how to accurately find heart disease. In 1994 he presented his original theory on Inflammation and Heart Disease in “The Pathogenesis of Vascular Disease,” (Textbook of Angiology, ed. John C. Chang, New York: Springer Verlag, 1999, 787-98) and presented on 20/20 in 2004. His research career has also involved investigating and correcting errors made in medical testing including coronary arteriography and nuclear imaging; for both heart disease and cancer. In 2017 after two decades of work he patented the first method capable of measuring regional blood flow and metabolic changes occurring inside the body. This method known as FMTVDM (Fleming Method) makes it possible to accurately determine what is happening inside the body as well as whether treatments prescribed for patients are working or not. In 2004 after reducing the amount of radiation he was giving patients for nuclear imaging tests of the heart he was accused of billing fraud. After evidence was hidden from the jury he agreed to a plea deal that did not state a crime making it possible for him to protect one of his children.
Richard Fleming, PHD, MD, JD: Is COVID-19 a Bioweapon? A Scientific and Forensic investigation, Skyhorse (7 Sep 2021, 176 pp.)By 1999, US Federal Agencies began funding Gain-of-Function research. Research that by its very nature is designed to increase the ability of pathogens to infect and harm people. In 2019, one of those pathogens was intentionally released upon the world in the Wuhan Wet Market. The key to proving and understanding this bioweapon is its spike protein. The very same spike protein now being made in millions of people after the COVID vaccines are injected into them. These vaccines are nothing more than the genetic code of this bioweapon. This book traces the publication and money trail of COVID-19; showing who is ultimately criminally responsible for the design and development of this weapon, which violates the Biological Weapons Convention (BWC) Treaty, exposing those who have committed crimes against humanity. Dr. Fleming will reveal the ultimate conspiracy: one that puts the future of the entire world at stake.
A brief 3+ minute overview of Is COVID-19 a Bioweapon? is presented by Dr. Fleming in Appendix 10. In Chapter 3 of his book, The Paper Trail of the US Funding for Gain-of-Function Research, Dr. Fleming cites a 7 February 2002 report by George Will from the Washington Post posted on the UCLA Dept of Epidemiology School of Public Health, “War and Health”. A salient portion of the report states:
... President Bush’s budget asks Congress to more than quadruple spending -- from $1.4 billion to $5.9 billion -- on bioterrorism. Last week Defense Secretary Donald Rumsfeld was unspecific in saying “it is likely” terrorist attacks “will grow vastly more deadly” than those of Sept. 11. But budgets often make government’s thinking clear, and the bioterrorism money may imply Rumsfeld’s meaning.Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases at the National Institutes of Health, says this infusion of money will accelerate our understanding of the biology and pathogenesis of microbes that can be used in attacks, and the biology of the microbes’ hosts -- human beings and their immune systems. One result should be more effective vaccines with less toxicity.
Dr. Fleming goes on to list citations of funding by US Executive Branch Agencies—beginning with the Department of Defense—from pages 31 thru 85. See the complete link-referenced list in Appendix 11. He concludes Chapter 3 with the summary:
Collectively these documents reveal, as shown in the appendix, that more than $61 million dollars in research funding was paid to Peter Daszak at EcoHealth, who then worked with Ralph S. Baric at the University of North Carolina, and Shi Zhengli at the Wuhan Institute of Virology, to conduct research on viruses including Gain-of-Function research on coronaviruses.
In the following December 2021 recording, Dr. Fleming gives sworn testimony regarding the following:
In the above, at 4:43, Dr. Fleming explains that, “The Biological Weapons Convention Treaty states that any adjustment or modification of a biological agent like this virus that doesn’t provide a benefit for mankind is a biological weapon.... [at 05:42] We’ve looked at all the different coronaviruses that exist on this planet. None of them have the PRRA insert, none of them have this tremendous amount of HIV insert, none of them have a Regional Binding Domain that is a prion-like binding domain which means that where it attaches to the cells is a prion-like domain and prions are things that are abnormal proteins that cause other proteins to become abnormally folded.”
Fleming’s May 2021 appearance on The Highwire covers a wide swath of context such as the following (emphasis added):
at 10:08
The first notation of a chimer, or a gain-of-function, for SARS-CoV-2 dates back to 2006 when a Chinese Lab combined Hepatitis C virus, HIV1, SARS-CoV-1, and SARS-CoV-2.† I found the research on it. This is an example that, the more you dig and the more data you find, the more you realize these people have been doing this with the express purpose of re-engineering and seeing what they could do. And Daszak’s papers, and Baric’s papers and Shi Zhengli’s papers repeatedly point out that they are making well known, infectious, pathogenic agents and they’re delighted with the fact. In fact in 2015, they came out and announced that they could produce a more virulent, pathogenic virus that would produce a pandemic. And yet they were still allowed to move forward on that.† Qiuying Huang et al. “Preparation of a Chimeric Armored RNA as a Versatile Calibrator for Multiple Virus Assays,” Clinical Chemistry 52, no. 7 (July 1, 2006): 1446-48 (PDF) and Supplement A, doi:10.1373/clinchem.2006.0699710 (PDF)
Chapter 5, An Intentionally Released Bioweapon, from Is COVID-19 a Bioweapon? opens with:
All too often, people believe that weapons are designed to kill people. I would argue quite the contrary. The best weapon doesn’t kill people; it devastates and demoralizes them. It reduces their will and capacity to wage war or to fight back. In battle, the best way to do that is to maim the enemy so their friends will come to their aid and leave the battlefield to shelter their friend.The best weapon to devastate a country is one that removes the will of the people to fight. It effectively diminishes the lifestyles of the enemy, reducing the security of life as the enemy knows it and replaces that security and freedom with fear and uncertainty. SARS- CoV-2 has done exactly that. It has devastated economies, removed the personal freedoms people were used to, reduced goods and services, and turned friends against friends and family members against family members. It has divided nations and people.
This past summer, 10letters.org was launched. It invites everyone to send a letter to each person’s State Attorney General demanding they convene a grand jury to bring criminal indictments against the perpetrators of “crimes against humanity employing Gain-of-Function research paid for by American taxpayers and conducted throughout the United States and other countries.” A seven-page Indictment Letter (local PDF copy), addressed to “State Attorney General, District Attorney, and/or Applicable Prosecuting Authority” by Dr. Fleming, summarizes the reason and purpose for convening a grand jury including the following segment:
The materials provided herein provide evidence that the aforementioned individuals and entities are guilty of the above noted crimes at the State, in addition to crimes at the Federal level, including but not limited to, Crimes of Conspiracy, Crimes Against Peace, and Crimes Against Humanity, for the Intentional, Knowing, Willful and Reckless violation of the following Treaties and accepted human Ethics:
(1) the 1947 Biological Weapons Convention (BWC) Treaty,For the individuals listed above, as well as those found to be criminally culpable following further investigation of these crimes, who have taken an Oath to Uphold and Defend the Constitution of the United States of America, and who have then violated these Treaty laws under Article VI of the U.S. Constitution, these individuals are also guilty of Treason.
|
“
|
Hundreds of millions of people have now been subjected to a “prototype” project by the Department of Defense under its Other Transactional Authority. The prototype project includes invention, production, supply chain mechanisms, and injection planning and performance.
|
|
— Atty Warner Mendenhall, Covid Injections: a DOD prototype project.
The prototype shot is government property until it is in your body. 5 Sep 2022 |
|
Contrary to much of the focus by the New Fourth Estate on the pharmaceutical cartel’s regulatory capture of NIH, NIAID, FDA, CDC, etc., it is the US military, the Department of Defense that has been in charge of the development, manufacturing, clinical testing, supply, production, and distribution of the mRNA vaccines. These shots are also the legal property of the DOD until they are injected into people.
Alexandra (Sasha) Latypova is a Soviet expat and pharmaceutical industry expert. Near the end of an October conversation with Tessa Lena [see: "Garbage Soup": Alexandra Latypova on Regulatory and Manufacturing Fraud in C-19 Injections], Latypova describes the following:
at 57:55
As I said before, I figured out that this was collusion with the FDA at least, between manufacturers and FDA and CDC. But what I had later learned—and this is now publicly available for a long time—but I had later learned that this is actually a DOD program and it's much larger than people realize. Here is the powerpoint from Vaccines and Related Biologicals Pfizer Committee meeting in October of 2020, so 2 years ago [conducted 22 Oct 2020]. And this is when they were setting up this Operation Warp Speed to manufacture these products. This is their own internal organizational chart:Now it's turned on the side but you can see that the Chief Operating Officer of the whole operation is the Department of Defense. And the Chief Science Officer is HHS and the FDA. How to read the org chart: these are the people in charge; US Government, DOD, HHS—actually DOD and HHS are merged into the same entity under the public health emergency that was announced by Alex Azar in early 2020. We still have that public health emergency which was recently extended—I don't know—eleven, twelve times—just recently got extended again. Even though there is no emergency. Nobody is dying of Covid really, hardly any covid around. In most of the United States there is practically none and we still [are] extending these public health emergency and we still have this organizational structure in place. But as you can see, as far as the vaccine manufacturing, the government is in charge. Specifically the Department of Defense is the head of this and they're in charge of manufacturing and all that. And then pharmas are really down below on their organizational structure. They are just commandeered by the US Government to produce these things. But they have no say. But they're getting a lot of money so they're happy and they're producing what the government tells them. As you can see here the government runs clinical trials, the government does supply, production, distribution, manufacturing. And that's true—I found a lot of contracts made by the Department of Defense, BARDA [Biomedical Advanced Research and Development Authority], and HHS at the time of setting up this whole structure. And these contracts are very specific about this. I read dozens of them, there are hundreds of them. People don't realize that—we all talk about Pfizer and Moderna and maybe Jannsen, but there are dozens and dozens of vaccine manufacturers that the DOD has set up, for a long time and had that infrastructure in place way before this public health emergency that they announced.
As you can see here the government runs clinical trials, the government does supply, production, distribution, manufacturing. And that's true—I found a lot of contracts made by the Department of Defense, BARDA [Biomedical Advanced Research and Development Authority], and HHS at the time of setting up this whole structure. And these contracts are very specific about this. I read dozens of them, there are hundreds of them. People don't realize that—we all talk about Pfizer and Moderna and maybe Jannsen, but there are dozens and dozens of vaccine manufacturers that the DOD has set up, for a long time and had that infrastructure in place way before this public health emergency that they announced.
That was all set up, in place, for many years, large capacities. And they also contracted with everyone: with therapeutics manufacturers, with diagnostics, with suppliers of masks, suppliers of diagnostic assays, different other products, and also staffing. For example, DOD contracted with ICON, who is supposed to be a subcontractor of Pfizer, to run clinical trials. But DOD contracted with them directly.
So DOD had the control of how those clinical trials were going to be run. So my question is, Who is REALLY manufacturing these products? The obvious answer here is that the Department of Defense both designs, makes, produces, distributes these products. And by the way, in the United States the vials are property of the Department of Defense until they get injected into somebody.
Again, people don't realize this but Department of Defense makes this thing, manufactures it, directed everything, research and clinical trials. Pharmas are there just as a front and the pass-through entity for the money. But it's entirely property of DOD, all of it.
In fact, in the contracts they also absolve everyone of responsibility under the PREP Act. So as long as you followed Department of Defense’s orders in injecting people with this you don't have to provide informed consent. You don't have to follow any rules. You can be [an] untrained person from a Fire Department, inject somebody, hit their blood vessel directly, poison them, kill them, and you will have no responsibility whatsoever as long as you followed Department of Defense’s orders. Then you are absolved of any liability and the last sentence of that clause says that is “both civilian and military applications.”
end 1:03:12
From the above regarding US DOD contracting with many, many vaccine manufacturers, see the massive listing, COVID-19 Contracts, at Knowledge Ecology International, Attending And Mending The Knowledge Ecosystem.
For the quotation in the last sentence above, which reads in full, “The items and technology covered by this Contract are being developed for both civil and military applications.”, see page 42 in DoD/ASPR/BARDA-Moderna Contract W911QY20C0100. August 9, 2020.
For the statement that the vials are DOD property see Attorney Warner Mendenhall, Covid Injections: a DOD prototype project. The prototype shot is government property until it is in your body., CovidLawCast.Com, 5 Sep 2022.
An Operation Warp Speed org chart from 30 July 2020 details more specifics about DOD and HHS command and control structure of the C19 experimental injections program:
In 2012, DOD’s Defense Advanced Research Projects Agency (DARPA) began investing in the development of gene-encoded vaccines, a new category of preventive measures based on DNA or RNA. See ADEPT:PROTECT - Advancing National Security Through Fundamental Research; https://www.darpa.mil/attachments/ADEPTVignetteFINAL.pdf (local PDF). The Federal Contract Opportunities for DARPA’s program, “Autonomous Diagnostics to Enable Prevention and Therapeutics: Prophylactic Options to Environmental and Contagious Threats” (ADEPT-PROTECT), was posted on 1 November 2012. The Summary states:
Federal Contract Opportunity for Autonomous Diagnostics to Enable Prevention and Therapeutics: Prophylactic Options to Environmental and Contagious Threats (ADEPT-PROTECT) DARPA-BAA-13-03. The NAICS Category is 541712 - Research and Development in the Physical, Engineering, and Life Sciences (except Biotechnology). Posted Nov 1, 2012. Due Jan 15, 2013. Posted by the Defense Advanced Research Projects Agency (DOD)
|
“
|
The truth is that DARPA, which is the operational development arm, basically the CIA, fell in love with the RNA technology over a decade ago. They decided to capitalize it and force it into the market space. For instance, they're the ones that have capitalized through In-Q-Tel, their investment arm, the new RNA manufacturing facilities up in Canada. This is a CIA program. There's no ambiguity here. I'm not telling state secrets.
The technology was basically pulled out of the trash can, because it had been suppressed by Merck after I developed it over 30 years ago. Then it was advanced very aggressively by DARPA. DARPA funded and basically built Moderna. They're continuing to push all this. They're pushing it through the government. What you're seeing is the power of the intelligence community and the new bio-defense industrial complex that's developed since the anthrax attacks and it really goes beyond that in being able to push their agenda through the government.
—Robert W Malone MD, MS, mRNA Vaccines: The CIA and National Defense, Who Is Robert Malone, 27 Oct 2022
|
The laws passed or modified by Congress have provided the authority to both the DOD and HHS cited above by Sasha Latypova. Katherine Watt is a self-described Roman Catholic, American, Gen-X writer, paralegal, printmaker, wife and mother. She founded Baliwick News as an independent newspaper in 2016. The name reflects “the sociopolitical, economic and legal status of the American people as peasant subjects in a neo-feudal, global jurisdiction of control and oppression; we are no longer sovereign citizens of a functioning Constitutional republic.” Her critical analysis of US law and history of legislation is formative and profound. Charles Rixey writes of Katherine Watt, “Excellent coverage of the legal implications of the pandemic”. As Watt describes her research and writing focus:
I work on finding, reading, analyzing and reporting on statutes and regulations passed by US Congress, and executive orders and legislation signed by US presidents, implemented by US Health and Human Services secretaries and Secretaries of Defense, mostly since 1983, and on judicial decisions by federal and state courts, as criminal acts of treason that built the legal foundations for the unconstitutional, democidal American public health-police state, which was deployed fully for the first time on January 31, 2020 with HHS Secretary Alex Azar’s declaration of public health emergency on the Covid-19 pretext.
A discussion between Sasha Latypova and Katherine Watt on 4 Nov 2022 centers on Watt’s analysis in American Domestic Terrorism Program published in April 2022 with ongoing updates. An annotated transcript of this recording reflects the wide scope of research and analysis produced on Bailiwick News including the following summary about a very special arrangement called an Other Transaction Authority that is “a separate contracting, purchasing framework that US government agencies can enter into with private companies.” As described by Katherine Watt:
I came across it because of Brook Jackson’s case. Brook Jackson is the whistleblower who was working for Ventavia, who was a subcontracted to Pfizer under the contract Pfizer had with the Department of the Defense to produce a hundred million doses of what they call a vaccine and distribute it through the DOD to all the people in the United States. Brook Jackson, as soon as she got to her trial site—she had three—in Texas, she noticed there were terrible problems with the clinical trials. She reported it first to her bosses at Ventavia, then to people at Pfizer. Then she tried to file, I think an anonymous hotline report, to the FDA and within hours of the FDA report, she was fired. Then she filed a False Claims Act case because her theory at that time was that Pfizer was defrauding the US government by falsely saying they were doing good clinical trials, and that the US government would want to know this because they would want to not spend money on a fraudulently produced product.It turned out that that is not the case. The US government was in on the fraudulent clinical trials and in on the whole fraud entirely. That came out in Pfizer’s April 2022 motion to dismiss. Because Brook, when she filed her False Claims Act, she attached the Statement of Work, which was a contract that was supposed to govern how the clinical trials were done. And in its motion to dismiss Pfizer attached another contract called an Other Transaction Authority—OTA contract—saying in effect, no, we had no obligation to conduct valid clinical trials because the only goods and services we were providing to the US government, according to this contract are a large scale manufacturing demonstration for a prototype. So they split off the clinical trials from the manufacturing and production side. I looked at that contract and had already come to the conclusion that it was a joint fraud between Pfizer and the DOD. And this corroborated that in Pfizer’s own words.
So the OTA is a separate contracting, purchasing framework that US government agencies can enter into with private companies. And the report that I sent you is from KEI. The title of it is Other Transaction Agreements: Government Contracts that Eliminate Protections for the Public on Pricing, Access and Competition, Including in Connection with COVID 19 Vaccines and Treatments [KEI Briefing Note 2020: 3 Other Transaction Agreements: Government Contracts that May Eliminate Protections for the Public on Pricing, Access and Competition, Including in Connection with COVID-19; local PDF]. It started in 1958, according to that report through NASA. But it’s since been expanded to, I think they said, 11 agencies have it now, have this special authority that Congress has given them to enter into these contracts. And it suspends all kinds of oversight.
That’s the bottom line of what an OTA does. In my view, Pfizer is probably correct that under the terms of the OTA, they had no obligation to ever conduct a valid clinical trial. They could make the entire thing a fraud. They could make the entire thing seem to be real and said that actual data, but it didn’t have to be good data. It didn’t have to be in compliance with any of the regulations that otherwise govern clinical trials. That’s why in the one piece I’ve done on it, I compared it to the Emergency Use Authorization because OTA did for the financial contracting side, what EUA did to the drug regulation side: they both just took them out of the normal.
See Appendix 12 for a list of the bulk of Bailiwick News research and analysis mostly from 2022. As one instance (of so many) of Katherine Watt exercising her intelligence and wisdom with clarity and coherence, see Biotech idolatry: DOD-Pfizer contracts have replaced federal constitutions and laws - And the DOD-DOJ-HHS complex has replaced federal legislatures and courts. 14 Sep 2022.
Charles Rixey self describes as “Investigating Covid’s origins with DRASTIC, a Marine, father, husband, Roman historian, & Covid-19 Analyst [who] spent 15 years as a CBRN/C-WMD Leader/Analyst/Instructor for USMC & DoS.” He writes at “Prometheus Shrugged, DRASTIC’s COVID-19 Origin Investigations - General Political & Data Analysis.” At the conclusion of Gaslight of the Gods, part VII: Allegory of the Plague - The true legacy of Anthony Fauci, 29 Jul 2022, Rixey includes his statement:
To Congress, & to the Biden Administration,To the left are my great-grandfather, grandfather & my uncles. I added them here for emphasis, because it’s important to understand that the big-picture implications in The Myth of the Blind Watchmaker are real - & serious. It’s against that backdrop that I am compelled to stand up & speak truth to power:
In late January & early February of 2020, Anthony Fauci, Francis Collins & Kelvin Droegemeier spent far more time shaping the SARS-CoV-2 origin narrative than preparing for the actual pandemic. Immediately following the release of a scientific pre-print from India that noted HIV-1 inserts in the SARS-CoV-2, immediate action was taken to suppress awareness of those inserts and of the furin cleavage site.
There was no action taken to alert medical personnel of the existence of the furin cleavage site – the insert that made SARS-CoV-2 one of the most infectious viral pathogens in human history. This fateful decision is both the most obvious & the least known pandemic failure amongst the citizens of the world; it delayed the global response and erased any chance of preventing what followed.
The symptoms of Long COVID are the harvest we’re now reaping from the seeds sown over the course of a single week in late January & early February of 2020, via decisions made by the officials entrusted to protect us. They chose to protect themselves. This is true no matter whether SARS-CoV-2 came from a bat or the hands of a master craftsman.
There is no national security interest that rises above the need for justice for a million American victims of the COVID-19 pandemic – regardless of who is to blame for its emergence. There is no public health statute that allows for censorship as a means of obstruction of justice, which is exactly how the practice has been employed. You cannot violate the Constitution under any law, much less as a means to avoid prosecution for violating some other law.
Here, on Memorial Day, 4 of those 5 men pictured observe Capitol Hill from the slope below Lee House hill in Arlington National Cemetery. Neither they nor the million dead Americans can voice their disgust, so I must speak for them. So be it.
|
“
|
The goals and actions of the individual humans working on the global Covid-19 democide project are so brazenly and profoundly evil that good human minds shut down the instant they confront the information. We recoil instinctively—emotionally, cognitively and spiritually—from the extraordinary saturation of evil; we struggle to grasp how it can be so comprehensive in its scope and destructive in its force.
—Katherine Watt, Legal Walls of the Covid-19 Kill Box, 26 Feb 2022
|
In the Introduction to History Will Not Absolve Us, the author emphasizes the essential requirement of a desire to know for someone to acquire knowledge.
Knowledge is not something which everyone wants. It is difficult to acquire, and in order to know, one must have a desire to know. In turn, one’s desire to know depends on social attitudes and social activity. To acquire knowledge one must go through the laborious process of digesting the work of others and make it one’s own. One can be helped to acquire knowledge and be guided in the process, but one cannot be given it directly. The process of acquiring knowledge has no true beginning. As with life one enters in the middle of the process and must attempt to go back and pick up what has been worked out historically while at the same time carrying the process forward.
In the opener, Gaeton Fonzi quoting Marty Schotz refers to people in the US generally, and in the US government specifically, not wanting to know that the assassination of the 35th President was a conspiracy organized, carried out, and covered up by members of the national security state structure codified in the National Security Act of 1947.
... one of the primary means of immobilizing the American people politically today is to hold them in a state of confusion in which anything can be believed but nothing can be known, nothing of significance that is.... And the American people are more than willing to be held in this state because to know the truth—as opposed to only believe the truth—is to face an awful terror and to be no longer able to evade responsibility. It is precisely in moving from belief to knowledge that the citizen moves from irresponsibility to responsibility, from helplessness and hopelessness to action with the ultimate aim of being empowered and confident in one’s rational powers.An indicator of how debauched the public square has become over the past half-century, is the fact that today, what so many people believe has almost nothing to do with knowing the grim horror of what has been inaugurated since early 2020. While a genuine pandemic of fear was proclaimed and perpetrated by a tightly connected group of people, the man-made SARS-CoV-2 bioweapon was not invincible. Efficacious early treatment protocols being identified by that summer put the lie to the psychological operation being conducted globally. For a sampling of analyses evaluating this unspeakable psyop see:
Memo re: US federal law on bioweapons reclassified as public health measures. (45 pp.)
NUTSHELL:US Government since 1969 has incrementally transferred/hidden the joint DOD+HHS Chemical and Biological Warfare Program (50 USC 32) in the Public Health Service Act (42 USC 201) and Food Drug and Cosmetics Act (21 USC 9), such that federally-funded, federally-directed public health programs and products are actually bioterrorism programs and biological and chemical weapon attacks.Much more information available.The government's purpose is to commit mass murder/depopulate the world, without public knowledge and without legal consequence, and enslave survivors for wealth and power centralization through digitized 'vaccine' passports and digital currencies, without public knowledge and without public resistance.
Herein:
p. 2 - SECTION 1 - June 2022: Covid-19 countermeasures as a case study[1] of the EUA legal status that pseudo-converts biowarfare weapons and programs to medical products and public health programs.
p. 6 - SECTION 2 - Timeline of federal statutes involved, from 1969 to present, related to US government-directed administration of toxic products on non-consenting human beings, excerpted from April 2022 American Domestic Bioterrorism Program[2] post.
p. 25 - SECTION 3 - Sept. 28, 2022 report on the evolution of requirements related to DOD reporting on CRBN programs to Congress.[3]
p. 32 - SECTION 4 - Oct. 19, 2022 - Other Transaction Authority (OTA) is to federal procurement contract regulation as Emergency Use Authorization (EUA) is to federal drug safety regulation.[4]
p. 41 - SECTION 5 - Oct. 25, 2022 - Condensed summary of the legal nightmare for judicial review.[5]
[1]
https://bailiwicknews.substack.com/p/covid-19-injectable-bioweapons-as
[2]
https://bailiwicknews.substack.com/p/american-domestic-bioterrorism-program
[3]
https://bailiwicknews.substack.com/p/dod-chemical-and-biological-warfare
[4]
https://bailiwicknews.substack.com/p/other-transactional-authority-ota
[5]
https://bailiwicknews.substack.com/p/pharmaceuticidal-tendencies
|
“
|
... why do I say the hospitals are murdering people? Because I’m involved in trying to get people out of them. As part of my analysis, in trying to help people escape the ICU intensive care, I’ve stumbled on a variety of things that are really quite interesting from a legal perspective. And that is that in 2008, the US Government merged Public Health with Law Enforcement, with the Judiciary and with Corrections. All four of them are now under one roof....
My client went in with an aneurysm. The client was nonetheless treated in the exact same format I’m telling you about: with the Midazolam, with the Remdesivir. They put him in the Covid ward. They never had Covid. But what they did, instead, was they they doped him up on morphine and fentanyl and a variety of a cocktail of drugs. I called the hospital’s lawyer and said, Listen, we want to move him to other care. And the hospital’s lawyer told me, No, your client is going to die in our hospital. This was his words....
|
|
—Atty Todd Callender, Open Secrets, Corona Committee, 25 Mar 2022
|
|
While Fauci and Collins are explicitly listed, primary perpetrators HHS Secretaries Alex Azar and Xavier Becerra must also be called out as identified by Katherine Watt’s exhaustive research and analysis. In Legal Walls - SHORT VERSION - Worldwide Schrodinger’s nation-states and people: simultaneously sovereign and not-sovereign, citizens and slaves. (21 Mar 2022), Watt writes:
Angry American citizens and elected representatives have been trying to use the criminal and civil courts to stop the governmental and corporate abuse of citizens and hold the perpetrators accountable for the crimes they’ve already committed, since at least May 7, 2020. Filed cases include:
- 2020/05/07 - Butler et al. v. Wolf et al., 2:20-cv-677-WSS, filed in Pennsylvania under 42 USC §1983 - Civil action for deprivation of rights. District Court found in favor of plaintiffs. Third Circuit Court of Appeals overturned/reversed District Court and then dismissed appeal as moot. Supreme Court refused to hear plaintiffs’ appeal, by rejection dated 01/11/22. (Bailiwick synopsis of Pennsylvania cases posted 02/04/22.)
- 2021/01/08 - US-DOJ/Brook Jackson v. Pfizer et al., 1:21-cv-00008-MJT, filed in Texas under 31 U.S. Code §3729 - False Claims Act. [Exhibits] Whistleblower gagged; case postponed indefinitely. [See Brook Jackson - Pfizer Whistleblower, Totality of Evidence]
- 2021/07/21 - America’s Frontline Doctors v. Becerra et al., 2:21-cv-00702-CLM, filed in Alabama, under 21 U.S. Code §360bbb - Expanded access to unapproved therapies and diagnostics.
- 2021/08/21, Ealy, Linthicum and Thatcher v. Redfield, Walensky, Azar et al., 3:22-cv-356-HZ, filed in Oregon, under 18 USC § 3332. Amended petition to impanel special grand jury to investigate federal crimes filed 03/07/22. The petition states there is “probable cause to believe one or all Defendants violated the...Administrative Procedures Act (5 U.S.C. §551 et seq.), the... Paperwork Reduction Act (44 U.S.C. §§ 3501-3521, Public Law 96- 511, 94 Stat. 2812 amended to 44 U.S.C. §§ 3501-3521, Public Law 104-13, 109 Stat. 182), and the...Information Quality Act (Section 515 of the Congressional Consolidated Appropriations Act, 2001 Public Law 106-554). In violating these federal laws, the Petitioners allege that crimes have been committed against the citizens of the United States...there is probable cause to believe that the violations of the APA, PRA, and IQA subsequently led to violations of the following federal laws by the Defendants, Major Fraud Against the United States (18 USC §1031), Fraud in Connection with Major Disaster or Emergency Benefits (18 USC §1040), Conspiracy to Defraud the United States (18 USC §371), False Statements Related To Healthcare Matters (USC §1035), False Statements (18 USC §1001), False Information & Hoaxes (18 USC §1038), that can be constituted as acts of Domestic Terrorism (18 USC §2331 - Chapter 113B) and Malfeasance (18 USC §3333), that may have resulted from a Conspiracy Against Rights (18 USC §241) and definitely led to the Deprivation of Rights Under Color of Law (18 USC §242) and may include Subornation of Perjury (18 USC §1622) and Misprision of Felony (18 USC §4) to be determined during the investigation by the grand jury.
- 2022/01/17 - Boteler v. Fauci, Gates, Rockefeller, et al. Filed in Texas Office of Attorney General. No case number assigned.
- 2022/03/03 - Griner v. Biden et al., 2:22-cv-00149-DAK, filed in Utah under 5th and 14th Amendments to US Constitution.
These constitutional, civil and criminal cases have been blocked — by the American government and American judges — from moving to discovery, trial and adjudication. In other words, since Jan. 30, 2020, in the United States and most other countries, government murder of citizens (democide) has been legalized. And self-preservation and lifesaving of others have been criminalized.
At some point, it will become clear to a wider segment of the American population that for more than two years now, we’ve already been ruled over by a global organized crime syndicate. Law enforcement and courts are not going to save us. We have to understand that reality, and we have to respond to it.
See also, CJ Hopkins on Ukraine-Russia: Revenge of the Putin-Nazis:
“What is happening in Ukraine is, Russia is not playing ball. For some reason, it does not want to be destabilized, and restructured, and privatized by GloboCap. It is acting like a sovereign nation state ... which it is, and isn’t, which paradoxical fact GloboCap is trying to impress on Russia, just as countries throughout the global-capitalist empire impressed it on us for the past two years, as Trudeau impressed it on those protesters in Ottawa when he cancelled their rights and went full-fascist.
What is happening is, Russia is rebelling against GloboCap, and, unlike the other rebellious parties that GloboCap has been dealing with recently, Russia has thermonuclear weapons.”
The catastrophic deadliness of the products marketed as C19 vaccines, their inefficacy at infection control, their severe adverse effects—including debilitating and fatal damage they cause to human neurological, cardiovascular, reproductive, and immune systems and organs—combined with the disruption of the social fabric of global society, are blaring indicators of the intentional adoption of a top-down system of dictatorial control being directed and manipulated by present-day bad, nay evil, actors.
In US federal crimes for which there is evidence to prosecute Covid-19 bioterrorists who occupy US government positions, Katherine Watt summarizes how “judges will need to examine whether the credible evidence demonstrates that government directives establishing mass testing programs, hospital and nursing home death protocols and bans on early treatment are public health emergency measures, or whether they are prohibited acts under US and international law. They will need to examine the evidence and decide whether the US government’s recommendations, authorizations, mandates, masks, tests and genetic spike protein/lipid nanoparticle injections are public health measures, or whether they are prohibited biological and chemical weapons and war crimes under US and international law.”
She goes on to delimit some “of the federal crimes implicated by Covid-19—43 are listed as of 21 Nov 2022—, plus a starter list of the US Government officials who should be investigated, arrested, charged and tried.... Men and women who are currently occupying high-level positions in US government or collaborating private sector entities, or who occupied such positions earlier in the development and deployment of the global Covid-19 bioterrorism campaign. Last updated 08/10/2022.”
Event 201, the high-level pandemic exercise, was conducted on 18 Oct 2019. Hosted by the Johns Hopkins Center for Health Security in partnership with the World Economic Forum and the Bill and Melinda Gates Foundation, it was “a 3.5-hour pandemic tabletop exercise that simulated a series of dramatic, scenario-based facilitated discussions, confronting difficult, true-to-life dilemmas associated with response to a hypothetical, but scientifically plausible, pandemic.”
On 23 October 2022, the Johns Hopkins Center for Health Security in partnership with the World Health Organization and the Bill and Melinda Gates Foundation conducted:


|
|
“
|
Fear and propaganda were the psychological weapons the Nazis used to impose a genocidal regime. And today, some are beginning to understand why the German people didn’t rise up. Fear kept them from doing the right thing. Medical mandates today are a major step backward toward a fascist dictatorship and genocide. Government dictate medical interventions; these undermine our dignity as well as our freedom....
The stark lesson of the Holocaust is that whenever doctors join forces with government and deviate from their personal, professional, clinical commitment to do no harm to the individual, medicine can then be perverted from a healing humanitarian profession to a murderous apparatus. The reason that the Greeks made their students of medical schools, before they were allowed into medical school, to swear the Hippocratic Oath was because they knew that in medicine, you gain knowledge about how you can actually kill and they had to promise that they would do no harm otherwise they weren’t allowed in medical school. I think they were ahead of us in understanding human nature.
What sets the Holocaust apart from all other mass genocides is the pivotal role played by the medical establishment, the entire medical establishment, every step of the murderous process was endorsed by the academic and professional medical establishment. Medical Doctors and prestigious medical some societies and institutions lent the veneer of legitimacy to infanticide, mass murder of civilians. T4 was the first industrialized medical murder project in history. The first victims were disabled German infants and children under three. They were identified by midwives who reported their existence to the state. The next victims were the mentally ill followed by the elderly in nursing homes. The murderous operations were methodical and followed protocol very, very carefully.
|
|
—Vera Sharav, The Roots of Evil, Corona Committee, 19 Mar 2022
|
|
For decades I’ve wondered, How did they do it on other planets? How did a self-aware and self-directed species, that was the predominate tool-maker, evolve beyond its adolescent coming-of-age phase and truly learn to live in peace within each soul, with each other, and with all life exploring itself on that globe? A second question arose in the 1970s and '80s when studying the assassination of President Kennedy and the health effects of low-level ionizing radiation: How is it that some people possess the antidote to official mind-numbing narratives such as A Lone Nut Assassin Changed History and There’s A Safe Level Of Exposure To Man-Made Radioactive Matter?
George Santayana’s insight about repeating the past is reflected in context of the work, Reason in Common Sense from The Life of Reason:
Progress, far from consisting in change, depends on retentiveness. When change is absolute there remains no being to improve and no direction is set for possible improvement: and when experience is not retained, as among savages, infancy is perpetual. Those who cannot remember the past are condemned to repeat it. In the first stage of life the mind is frivolous and easily distracted; it misses progress by failing in consecutiveness and persistence. This is the condition of children and barbarians, in whom instinct has learned nothing from experience. In a second stage men are docile to events, plastic to new habits and suggestions, yet able to graft them on original instincts, which they thus bring to fuller satisfaction. This is the plane of manhood and true progress. Last comes a stage when retentiveness is exhausted and all that happens is at once forgotten; a vain, because unpractical, repetition of the past takes the place of plasticity and fertile readaptation.In the present time, failure to retain lessons learned from the horrors of Word War II in Europe, are now globally condemning humanity to repeat unbridled evil. Last year, two letters by We For Humanity were published:
The August letter, addressed to Emer Cooke, Executive Director of the European Medicines Agency (EMA), opens with:
STOP HOLOCAUSTLadies and Gentlemen,
We, the survivors of the atrocities committed against humanity during the Second World War, feel bound to follow our conscience and write this letter.
It is obvious to us that another holocaust of greater magnitude is taking place before our eyes. The majority of the world’s populace do not yet realize what is happening, for magnitude of an organized crime such as this is beyond their scope of experience. We, however, know. We remember the name Josef Mengele. Some of us have personal memories. We experience a déjà vu that is so horrifying that we rise to shield our poor fellow humans. The threatened innocents now include children, and even infants.
In just four months, the COVID-19 vaccines have killed more people than all available vaccines combined from mid-1997 until the end of 2013 – a period of 15.5 years. And people affected worst are between 18 and 64 years old – the group which was not in the Covid statistics.
We call upon you to stop this ungodly medical experiment on humankind immediately.
What you call “vaccination” against SARS-CoV-2 is in truth a blasphemic encroachment into nature. Never before has immunization of the entire planet been accomplished by delivering a synthetic mRNA into the human body. It is a medical experiment to which the Nuremberg Code must be applied. The 10 ethical principles in this document represents a foundational code of medical ethics that was formulated during the Nuremberg Doctors Trial to ensure that human beings will never again be subjected to involuntary medical experimentation & procedures....
The September letter was sent to three national bureaucracies charged with regulating drugs and vaccines: EMA (EU), Medicines and Healthcare products Regulatory Agency (MHRA UK), and Therapeutic Goods Administration (TGA, Australia). These RED ALERTS were sounded more than one year ago to national agencies responsible for so-called public health. Given the magnitude of concern from ongoing consequences of injury and death and the continued efforts to inject these experimental drugs globally—with no genuine blinded trials and no long-term studies—one can only conclude it is willful intention to further imperil humanity’s birthright of natural immunity and to extinguish the future of the majority of humanity.
Most of today’s physicians working within the medical industry are caught up in the present-day lockstep as German doctors were more than 8 decades ago. A 2012 paper in the International Journal of Law and Psychiatry on Why did so many German doctors join the Nazi Party? explores an aspect of this. From the Abstract:
Given the medical oath to “do no harm,” many postwar ethical analyses have strained to make sense of these seemingly paradoxical atrocities. Why did physicians act in such a manner? Yet few have tried to explain the self-selected Nazi enrollment of such an overwhelming proportion of the German Medical Society in the first place. This article lends insight into this paradox by exploring some major vulnerabilities, motives, and rationalizations that may have predisposed German physicians to Nazi membership—professional vulnerabilities among physicians in general (valuing conformity and obedience to authority, valuing the prevention of contamination and fighting against mortality, and possessing a basic interest in biomedical knowledge and research), economic factors and motives (related to physician economic insecurity and incentives for economic advancement), and Nazi ideological and historical rationalizations (beliefs about Social Darwinism, eugenics, and the social organism as sacred). Of particular significance for future research and education is the manner in which the persecution of Jewish physician colleagues was rationalized in the name of medical ethics itself. Giving proper consideration to the forces that fueled “Nazi Medicine” is of great importance, as it can highlight the conditions and motivations that make physicians susceptible to misapplications of medicine, and guide us toward prevention of future abuse.
That no one authority in the FDA, CDC, NIAID, NIH, HHS, DOD will yet acknowledge nor address the inescapable anomalies and supreme, mind-bending contradictions that belie the “safe and effective” parroting of government and media talking heads should give one pause:
|
“
|
The intentional part—it’s fully intentional. But they ask me is it depopulation or genocide?
I can’t get into the head of a criminal. Nobody can. So, the purpose of why they’re doing this, I don’t know. But I know for sure it’s intentional. That’s what the data shows and that’s what their behavior shows and all the documents. Of course all these government officials in CDC and FDA and NIH, they all know. They all know how many people have died. They have great data to follow it. They’ve known it since day one. They followed thousands of deaths and they’re under no confusion about this. So the fact that they continue is just intentional.
|
|
—Sasha Latypova,
C-19 Injections, Regulatory and Manufacturing Fraud:
Tessa Lena Talks to Alexandra Latypova, 24 Oct 2022 |
|
Between July 2021 and August 2022, evidence of undisclosed ingredients in the COVID-19 “vaccines” was published by at least 26 researchers/research teams in 16 different countries across five continents using spectroscopic and microscopic analysis. Despite operating largely independently of one another, their findings are remarkably similar and highlight the clear and present danger that the world’s population has been lied to regarding the contents of the COVID-19 “vaccines”. This raises grave questions about the true purpose of the dangerous experimental injections that have so far been shot into 5.33 billion people (over two thirds of the human race), including children, apparently without their informed consent regarding the contents. Surprise findings include sharp-edged geometric structures, fibrous or tube-like structures, crystalline formations, “microbubbles”, and possible self-assembling nanotechnology. The blood of people who have received one or more COVID-19 “vaccines” appears, in case after case, to contain foreign bodies and to be seriously degraded, with red blood cells typically in Rouleaux formation. Taken together, these 26 studies make a powerful case for the full force of scientific investigation to be brought to bear on the COVID-19 “vaccine” contents. If the findings of these 26 studies are confirmed, then the political implications are nothing short of revolutionary: a global crime against humanity has been committed, in which every government, every regulator, every establishment media organization, and all the professions have been complicit.
Dr. Roger Hodkinson is a general practitioner and a medical specialist in pathology, a national pathology board examiner, and laboratory accreditation inspector. A graduate of Cambridge University and a Fellow of the College of American Pathologists (FCAP) and the Royal College of Physicians and Surgeons of Canada (FRCPC), he began voicing his concerns about our upside-down world in 2020. In the following 25 Aug 2022 recording, Why Is No One Talking About Sudden Dead Doctor Syndrome?, he speaks with Laura-Lynn Tyler Thompson (segment begins at 44:17 and runs to 1:23:56; mp3: 39:39). The following excerpts focus on the very future promulgation of the human species in terms of fertility and infertility in both women and men.
This has to stop, not just for children, but for the entire population. It’s the most catastrophic intervention in medical history. It’s at that scale of enormity.... As a pathologist with a very full, extensive career, I have opened up hundreds of uteruses that have come from the operating room. The gynecologists take it out. They don’t open it up. We do as pathologists in order to look at the pathology, to take sections and look at them microscopically. I can tell you that the endometrium is the lushest, most fragile tissue in the entire human body. You can put your finger in it, just like you can put your finger in the brain. It’s extremely delicate and it’s meant to be so as a nurturing environment for the develop—the fertilized ovum that comes down the fallopian tube and implants into the endometrium. The blood vessels in the endometrium are exquisitely fragile. Witness, how easy it is to make them bleed; a woman’s menstrual period every month. Those vessels are all lined by a receptor for the spike protein. The receptor is called the ACE2 receptor. So it should come as no surprise to hear of all these menstrual abnormalities that are happening after vaccination. Because the spike protein being massively overproduced in some women, hones in on many blood vessels, including the blood vessels in the lining of the uterus causing them to thrombose or bleed. Hence the reason for the menstrual abnormalities post vaccination, so called.But that’s merely the backdrop. That fertilized ovum that’s traveling down, hoping to be received by welcoming, lush endometrium, suddenly finds itself landing in a space that’s been devastated. Not at all welcoming. And so the likelihood of that ovum implanting and having a successful pregnancy is much lower. And that’s one of the principle reasons I think why we are seeing a decline in fertility for women. The other reason is that the spike protein—the antibodies directed against the spike protein—which is the intended consequence of this clot shot, those antibodies against the spike protein happen to cross-react to a particular protein in the placenta called syncytin. And that attack against the developing placenta would be another reason for the developing fetus not to survive.
But the story gets much, much more serious than that. Just a digression for a minute. Before getting into the developing female fetus. Spermatozoa counts have been dropping internationally for decades for reasons that are unclear. But we do know that superimposed upon that, there’s an additional 15% reduction in the concentration of spermatozoa following injection with the clot shot.... So that compounds the problem of course of infertility because that’s only the count by the way. It doesn’t reflect the actual viability and metabolism of an individual spermmatozoon. It’s simply the crude count. There may well be other functional abnormalities that are not being studied.
Anyway, to get to the big point, the big point is this: we know from the freedom of information requested for the Japanese as a result of the Pfizer [Biodistribution Report] submission there. That was done by Dr. Byram Bridle out of Guelph. We do know that that study that was presented to the Japanese and released very reluctantly by Pfizer, showed that nanoparticles without the mRNA inside them, just the naked particles, when injected into rats, those particles honed on the rat ovaries to a very significant degree. The third highest concentration in the rat was in the rat ovaries.
Now, baby girls are born with all the eggs they’re ever going to have in their entire life. They don’t make any more when they’re born. It’s about a million or so. And so each one of those ova is incredibly precious. So there could be an inflammatory attack going on against the ovary of a developing female fetus because we also know that nanoparticles of that size are well known to pass through what we call the placental barrier, the thing that keeps the baby safe from all kinds of noxious things. So these nanoparticles from the clot shot that are known to be inflammatory and known to concentrate in rat ovaries—by the way, not studied in humans, conveniently—despite knowing that those nanoparticles known to be inflammatory are getting through the placenta and could be, again, not studied, could be attacking the ovary of the developing female fetus. Translation: this may not be simply an effect on fertility. It could be causing infertility only manifest 20 years later when that little girl becomes of reproductive age. This is the scale. This is the scale of stuff that is still not studied, things with gigantic consequences. The only saving grace is that it seems, at least in the states, that parents are smartening up and are choosing not to get their children vaccinated.
|
“
|
Because the US Constitution was so ingeniously framed, the American people lived in a free republic for over two centuries. Sometime during the last ten years or so, we lost sight of the fact that the great advances our people have made in science, technology, and medicine were entirely predicated on free speech and the free exchange of ideas. James Madison, the author of our constitution, understood that the danger of infringing free speech greatly exceeded the danger of people making erroneous utterances. The reason for his conclusion is simple: The only way to correct erroneous perceptions and beliefs is to discuss and debate them. |
THE KEY that has locked everything up, making all the unspeakable, criminally unaccountable injury and death possible—right before everyone’s eyes—is the suppression of all information, analysis, and open debate about the wisdom and intelligence of so-called democratic governing policies. Censorship is the ultimate tool to smother and extinguish the free exchange of ideas and from this, the freedom to think. Robert Heinlein captured the essential power exercised by censorship in his 1949 novel, Revolt in 2100. The story revolved around efforts to overthrow a 100-year theocratic totalitarian United States of America:
I began to sense faintly that secrecy is the keystone of all tyranny. Not force, but secrecy ... censorship. When any government, or any church for that matter, undertakes to say to its subjects, “This you may not read, this you must not see, this you are forbidden to know,” the end result is tyranny and oppression, no matter how holy the motives. Mighty little force is needed to control a man whose mind has been hoodwinked; contrariwise, no amount of force can control a free man, a man whose mind is free. No, not the rack, not fission bombs, not anything—you can’t conquer a free man; the most you can do is kill him.
|
“
|
The thinking classes in America want to emulate the theocratic lunacy of the Sixteenth Century. They have become everything they used to despise as cruel, unjust, and crazy.... Our authorities have disgraced themselves behind a new theology of degenerate “science” that veers back into superstition and necromancy. Proof that they don’t believe their own story shows in their desperate efforts to hide the data, confabulate numbers, ignore true facts, and lash out viciously at anyone who discloses their zealous deceits.
—James Howard Kunstler, American Inquisition, Clusterfuck Nation, 17 Oct 2022
|
Hrvoje Morić is the host and producer of Geopolitics and Empire, an information-and-analysis-rich source. He “conducts interviews with prominent international experts on a wide-range of topics. The broadcast seeks to gain insight from guests who come from the left, right, and beyond. The host does not always agree with beliefs espoused by podcast invitees, but maintains an open mind, and believes it important to respectfully listen to a multitude of voices and let listeners come to their own conclusions.” As Hrvoje Morić states at the end of James Roguski: IHR Amendments Are WHO’s Backdoor to Global Control (15 Dec 2022),
“The e-mail list and website are our last lines of defense. We’re being censored and de-platformed. It’s almost impossible to find Geopolitics and Empire on the google search engine. We’ve been blacklisted. Youtube frequently strikes videos. Facebook restricts our page. Reddit, Twitter, and LinkedIn take down posts. After the Associated Press mentioned Geopolitics and Empire in a 2021 article co-written with NATO, or the Atlantic Council, our Patreon Account was terminated. Vimeo also terminated our Pro Account at one point. In April 2022, the Department of Homeland Security had PayPal ban us for life. The best free way to help Geopolitics and Empire is to leave a review on Apple Podcasts or elsewhere and subscribe to all of our media channels. You can find the video broadcasts now on five platforms: odysee, rokfin, rumble, bitchute, and brighteon. You can the audio broadcast on the entire podcast ecosystem: Soundcloud, Apple, Spotify, and so on. My current favorite social media channels are Twitter and Telegram but you can also find us on Gab, MeWe, Minds, Flote, VK, Instagram, Facebook, and LinkedIn....
Appendix 13 contains a selection of reporting and analyses on the censorship iron curtain including the marriage made in hell by USG with BIG tech. Of the many noteworthy signposts included, the following provides some of the core dynamics of collusion between the Executive Branch of the US Government and the Lords of Digital Communication.
Fauci’s Red Guards: Lawsuit Reveals Vast Federal Censorship Army - “This evidence suggests we are uncovering the most serious, coordinated, and large-scale violation of First Amendment free speech rights by the federal government’s executive branch in US history”, Michael P Senger, The New Normal, 2 Sep 2022One aspect of dictatorships that citizens of democratic nations often find puzzling is how the population can be convinced to support such dystopian policies.... How can they get so many people to support policies that, to any outsider, are so needlessly destructive, cruel, and dumb? The answer lies in forced preference falsification. When those who speak up in principled opposition to a dictator’s policies are punished and forced into silence, those with similar opinions are forced into silence as well, or even forced to pretend they support policies in which they do not actually believe.... No regime in American history has ever previously had the power to force preference falsification by systematically and clandestinely silencing those critical of its policies. Until now.
More than 45 years ago Jerry Mander drew up a list of what would be Eight Ideal Conditions for the Flowering of Autocracy with the frame being: “Imagine that like some kind of science fiction dictator you intended to rule the world. You would probably have pinned over your desk a list something like this:
Over past decades, the Gain-Of-Function research and development by the US Department of Defense, combined with development of legal structures to nullify Constitutional rights of redress, set the stage for the 31 January 2020 declaration of a Public Health Emergency by HHS Secretary Alex Azar. Thirty years ago, the 1992 UN Earth Summit in Rio de Janeiro began to openly promote a “green” solution to further economic development. THE EARTH BROKERS: Power, Politics, and World Development (1994) is an account of what actually occurred in Rio by Pratap Chatterjee, then Global Environmental Editor of IPS, and Matthias Finger, then Associate Prof, Teachers College, Columbia Univ. The authors describe the Biodiversity Convention, as well as Agenda 21 in terms of the ongoing pursuit of global control of everything through economic domination (emphasis added):
[p.42] ... the biodiversity convention was generally considered the biggest success of the entire UNCED process. A total of 156 countries signed the convention in Rio, and four more have signed it since, but only six had ratified it as of February 1993. Many NGOs were indeed keen for the convention to be signed. While recognizing that it had many shortcomings, groups at a workshop held by the Brazilian NGO SOS Mata Atlantica (SOS Atlantic Forest) called the convention ‘a milestone in an ongoing process for the conservation and wise use of the world’s biodiversity’. The Third World Network, however, noting that last minute changes had been made to the convention’s provisions on ownership of genetic resources, advised Southern countries not to sign.[3] Amid the excitement of the Summit and the general anger with the USA’s pro-business stance, few noticed the warning. Indeed, the biodiversity convention is just one of many typical examples where the concern for exponential destruction of the world’s biodiversity has been perverted into a preoccupation with new scientific and (bio-)technological developments to boost economic growth. Or as Vandana Shiva puts it: ‘It is ironical that a convention for the protection of biodiversity has been distorted into a convention to exploit it’.[4] Though this is not surprising, given the conceptual framework of the Brundtland Commission discussed earlier, it is nevertheless worth while identifying the three key arguments that cement this perversion: first, the convention gives ‘nation-states the sovereign right to exploit their own resources pursuant to their environmental policies’,[5] thus transforming biological diversity into a natural resource to be exploited and manipulated. Then, the convention implicitly equates the diversity of life – animals and plants – to the diversity of genetic codes, for which read genetic resources. By doing so, diversity becomes something modern science can manipulate. Finally, the convention promotes biotechnology as being ‘essential for the conservation and sustainable use of biodiversity’.[6] ... the main stake raised by the biodiversity convention is the issue of ownership and control over biological diversity. In the case of the North, and the USA in particular, the major concern was protecting the pharmaceutical and emerging biotechnology industries ...
- V. Shiva, Third World Network Briefings, 1992, Paper No. 24, Third World Network, Penang, Malaysia, p. 80.
- Third World Resurgence, 1992,24/25, p. 16.
- Convention on Biological Diversity, 5 June 1992, article 3. (Obtainable from: UN Department of Public Information, attn. Project Manager for Sustainable Development, Room S-894, United Nations Plaza, New York, NY 10017.)
- Article 16(1), Convention on Biological Diversity, op. cit..
Ownership and control over genetic codes which modern science can manipulate to further the development of biotechnology became a primary area of research and development for the US military which went into overdrive after the 2001 anthrax attacks.
|
“
|
Genetic engineering biotechnology is an unprecedented alliance between bad science and big business which will spell the end of humanity as we know it, and of the world at large. Genetic engineering biotechnology is inherently hazardous, but the genetic-determinist mindset that misinforms both practitioners and the public takes hold of people’s unconscious, making them act involuntarily, unquestioningly, to shape the world to the detriment of human beings and all other inhabitants, |

|
“
|
Alright – we know there was an inquisition. And this
inquisition went on for 4 or 500 years in Europe. The purpose
of the inquisition was to alter the perceptional reality of the
descendants of the tribes of Europe. To make them believe and
see reality the way the church wanted them to believe and see
reality.
The church called it – they waged a war for possession
– for possession, this is important – they
waged a war for the possession of the souls of the godless
heathens. And to be a godless heathen you just didn’t
believe in god. It wasn’t a part of your reality. Or
another way of becoming a godless heathen was to question the
authority of the church to do this.
... And they killed as many people as they could in order to get the other ones to submit. So they killed as efficiently as they could with the technology they had at their disposal at that time. And because they created a rationalization as to why to do it, it just became as efficient as they could do. And at some point, the descendants of the tribes of Europe no longer knew what it meant to be a human being. They just didn’t know – they didn’t want to know. So the descendants of the tribes of Europe, in the end, had to love what they feared which was there to possess them. I think it messed up love in a lot of ways, that they haven’t unsorted yet.
—John Trudell, What It Means To Be A Human Being, 15 Mar 2001
|
The drive to control the thoughts, choices, and actions of people through declarations of so-called public health emergencies and emergency use authorizations is the present day result of a domination system that has been going on for more than five centuries. The possession and control of land and people outside Europe began in earnest with Vatican papal bulls of the fifteen century and royal charters of England. Since the 1970s, Shawnee/Lenape scholar Steven Newcomb has studied and analyzed the drive to conquer and subjugate Original Free Nations and Peoples in the Western Hemisphere through a doctrine of domination.
A great deal of this history is laid out in publications like European Treaties Bearing on the History of the United States and its Dependencies to 1648 published by in 1917 by the Carnegie Institution in Washington D.C. The 1452 Dum Diversas papal bull by Pope Nicolas V instructed King Alphonse of Portugal to find non-Christian lands and “invade, capture, vanquish, subdue,” “all Saracens, pagans, and other enemies of Christ,” “to reduce their persons to perpetual slavery,” and “to take away all their possessions and property”. The 1496 Patent Granted by Henry VII to John Cabot empowered Cabot to take possession in the name of the King of England of countries then “unknown to all Christians”.
In an 1803 private letter from President Thomas Jefferson to then-governor of Indiana Territory William Henry Harrison, Jefferson candidly expresses the underlying intentions of the nascent US empire regarding the future of Original Free Nations, existent on the continent for thousands of years before arrival of the Europeans.
... The decrease of game rendering their subsistence by hunting insufficient, we wish to draw them to agriculture, to spinning and weaving.... When they withdraw themselves to the culture of a small piece of land, they will perceive how useless to them are their extensive forests, and will be willing to pare them off from time to time in exchange for necessaries for their farms and families. To promote this disposition to exchange lands ... we shall ... be glad to see the good and influential individuals among them run in debt, because we observe that when these debts get beyond what the individuals can pay, they become willing to lop them off by a cession of lands. In this way our settlements will gradually circumscribe and approach the Indians, and they will in time either incorporate with us as citizens of the United States, or remove beyond the Mississippi. The former is certainly the termination of their history most happy for themselves; but, in the whole course of this, it is essential to cultivate their love. As to their fear, we presume that our strength and their weakness is now so visible that they must see we have only to shut our hand to crush them, and that all our liberalities to them proceed from motives of pure humanity only. Should any tribe be foolhardy enough to take up the hatchet at any time, the seizing the whole country of that tribe, and driving them across the Mississippi, as the only condition of peace, would be an example to others, and a furtherance of our final consolidation.
Jefferson’s juxtaposition of projecting “the termination of their history” as being “most happy for themselves ... to cultivate their love” and “we have only to shut our hand to crush them” with “all our liberalities to them proceed from motives of pure humanity only” indicate the mindset of a domineering, abusive nature cloaking itself in pleasant-sounding euphemism. “Stay safe” and “safe and effective” are present-day euphemisms of indirection equal to those of Jefferson and so many other vaunted icons of the so-called United States.
In 1823 what 15th-century European church and state termed the right of “discovery” was formally codified into US federal law with the Supreme Court ruling, Johnson & Graham’s Lessee v M’Intosh where it remains to this day. From the time of the papal bulls, The Doctrine of Discovery is fundamental to both the establishment of the United States as well as its continuing domination of people and land. It was invoked and validated as recently as 2005 in the US Supreme Court case, City of Sherrill v. Oneida Indian Nation wherein 1820s US Supreme Court decisions were cited as precedent for denying the Oneida Nation land claim. Footnote #1:
Under the “doctrine of discovery,” Oneida II, 470 U. S. 226, 234 (1985), “fee title to the lands occupied by Indians when the colonists arrived became vested in the sovereign—first the discovering European nation and later the original States and the United States,” Oneida /, 414 U.S. 661, 667 (1974). In the original 13 States, "fee title to Indian lands," or "the pre-emptive right to purchase from the Indians, was in the State."The decision was unanimous, written by Justice Ruth Bader Ginsburg, the most liberal judge on the bench.
In his 2008 book, Pagans in the Promised Land: Decoding the Doctrine of Discovery Newcomb demonstrates how US government officials have used religious concepts of Christendom, often unconsciously, to justify the taking of Native American lands and to deny the independence of Original Free Nations. Newcomb has decoded Doctrines of Domination from original Latin texts of the papal bulls and, in the way these conceptions of domination fit together, has assembled a Protocol of Domination Vocabulary. In the 3 May 1493 The Bull Inter Caetera a sentence reads, “sub dominio actuali temporali aliquorum dominorum Christianorum constitute non sint”. Newcomb describes it as meaning,
The word “governments” appears in the Inter Caetera. There’s a sentence that says, “We trust in Him from whom empires and dominations”—dominationes in Latin—“and all good things proceed ... But the English version doesn’t say dominations. It says governments. So dominaciones and governments are synonyms, translated from Latin to English. That’s how we know that singular “domination” is also “government” and they’re parallel there.

Speaking in 2017 on US Settler Colonialism and Its Inseparable Offspring, Attempted Genocide, Historian Roxanne Dunbar-Ortiz addresses Understanding Where the US Military Came From & What It Is, and how The United States is a thoroughly militarized culture, all the more dangerous because we don’t know it. Her 2014 book, An Indigenous Peoples’s History of the United States is an essential primer on the reality of US history:
US policies and actions related to Indigenous peoples, though often termed “racist” or “discriminatory,” are rarely depicted as what they are: classic cases of imperialism and a particular form of colonialism—settler colonialism. As anthropologist Patrick Wolfe writes, “The question of genocide is never far from discussions of settler colonialism. Land is life—or, at least, land is necessary for life.”She quotes Patrick Wolf on Settler Colonialism and the Elimination of the Native:The history of the United States is a history of settler colonialism—the founding of a state based on the ideology of white supremacy, the widespread practice of African slavery, and a policy of genocide and land theft. . . .
Writing US history from an Indigenous peoples’ perspective requires rethinking the consensual national narrative. That narrative is wrong or deficient, not in its facts, dates, or details but rather in its essence. Inherent in the myth we’ve been taught is an embrace of settler colonialism and genocide. The myth persists, not for a lack of free speech or poverty of information but rather for an absence of motivation to ask questions that challenge the core of the scripted narrative of the origin story. How might acknowledging the reality of US history work to transform society? That is the central question this book pursues.
As Deborah Bird Rose has pointed out, to get in the way of settler colonization, all the native has to do is stay at home.[5] Whatever settlers may say—and they generally have a lot to say—the primary motive for elimination is not race (or religion, ethnicity, grade of civilization, etc.) but access to territory. Territoriality is settler colonialism’s specific, irreducible element.The logic of elimination not only refers to the summary liquidation of Indigenous people, though it includes that. In common with genocide as Raphaël Lemkin characterized it,[6] settler colonialism has both negative and positive dimensions. Negatively, it strives for the dissolution of native societies. Positively, it erects a new colonial society on the expropriated land base—as I put it, settler colonizers come to stay: invasion is a structure not an event.[7] In its positive aspect, elimination is an organizing principal of settler-colonial society rather than a one-off (and superseded) occurrence. The positive outcomes of the logic of elimination can include officially encouraged miscegenation, the breaking-down of native title into alienable individual freeholds, native citizenship, child abduction, religious conversion, resocialization in total institutions such as missions or boarding schools, and a whole range of cognate biocultural assimilations. All these strategies, including frontier homicide, are characteristic of settler colonialism.
The consequence of the Doctrine of Domination is the increasing-to-the-breaking-point concentration of financial wealth and exercise of control in fewer and fewer hands. The Domination System that Original Free Peoples have been dealing with for over 500 years is now coming after the 99% on Mother Earth. Everyone’s birthright of free will and exercising one’s unique wisdom and intelligence is in danger of being subjugated, vanquished, captured, and, as has already occurred for many people, being extinguished and killed.
The Fear Pandemic is the fog of war, apparently serving the purpose of obscuring the bid to establish a genuine Digital Dark Age wherein subsequent campaigns are in the works to replace fiat currency with Central Bank Digital Currencies[†]/“Smart Money”, in concert with “Vaccine Passports”[1][2], Digital IDs[1][2][3], and Social Credit Systems[1][2][3] to cement the establishment of a techno logic top-down control global gulag.
|
“
|
The Covid-19 pandemic response was not based on sound medicine or science, and was not commensurate with the actual threat of the illness. Even if Covid-19 had proved to be as lethal as it’s falsely claimed to be, violating human rights and depriving individuals of personal autonomy are never the appropriate response to a pandemic. We must never let this happen again.
The Covid-19 pandemic revealed movements, led by globalists and wealthy technocrats, but also supported by many of our government and public leaders, to grasp power in ways that have the potential to destroy the foundations of Western civilization. There is a push toward global governance, in which all citizens are tracked and controlled in every aspect of their lives through digital identification, under the guise of preserving and distributing Earth’s resources in a more “equitable” manner.
—Lori Weintz, The Great Overreaction, Brownstone Institute, 18 Dec 2022
|
Five Small Stones Legal Network is a US-based network of attorneys, doctors, nurses, paralegals, research scientists, data analysts and others working to use legal systems to raise public and judicial understanding of the global cull now in progress, stop the cull and obtain relief for injured and killed victims and their families.We’re connected with attorneys and doctors in other countries, including Canada, UK, Australia, New Zealand and South Africa, and working to strengthen those cross-links.
The network is building a legal education and legal support tool-kit to help pro se plaintiffs file cases on their own behalf, because there are not enough lawyers in the world to handle the tsunami of injuries and deaths, and because millions of ordinary people using distributed legal knowledge will be harder for the globalists to shut down.
Two sites emerged from this. Five Small Stones was announced on 30 Sep 2022 as an interim, download-only website to get “user-friendly legal information and tools into the hands of sick and bereaved people”. On 6 Oct 2022, the primary 5 Small Stones site went live. It’s stated purpose is to provide “tools and resources to drive the entitled globalist overlords who have infiltrated and co-opted the American executive branch and administrative agencies, out of the US Government and out of our country. They have been working for 75 years to isolate, surround and remove us from power over our government.”
The two areas of focus are Election and Medical Integrity. Concerning elections and correctly identifying the goal, “Throw the Machines Out”, builds on the work of James and Kenneth Collier who, beginning in 1970, understood very clearly the paramount danger of entrusting the US vote count to electronic systems owned by private corporations. Their daughter, Victoria Collier, wrote about this in A Brief History of Computerized Election Fraud in America (25 Oct 2003). In Military Medical Martial Law, the unthinkable danger of NEW Quarantine Powers Legislation cannot be overstated. While I do not resonate with all perspectives presented in 5 Small Stones (for example, the declaration of being “a patriot” appears to miss acknowledging the reality of US history), it seems that truly dispensing with meaningless distractions such as left-right, black-white, democrat-republican, conservative-liberal, will be essential IF there is to a genuine RESET of power to all people. A good source of inspiration—as Benjamin Franklin was exceedingly aware of and inspired by—are the Hau de no sau nee, (Six Nations), the oldest, living, participatory democracy on Mother Earth.
Beyond simply stopping the advancing snuffing out of inalienable human rights by global totalitarian digital dictatorships, it is life-and-death critical to envision what the future of our species CAN imagine, CAN create, CAN manifest, CAN establish for our children’s children’s children and ALL LIFE exploring itself here on Mother Earth. Every one of us has been gifted with these utterly mysterious and wondrous lives, existing in this supremely vital moment of Life on this planet, called here to actively participate in what John Judge described in 2002:
...the way you end what you’re calling terrorism is to restore justice, is to restore hope and then the sanction and the support for violence in those communities diminishes and it goes away. Because instead you have the sort of natural, civil and community structure that all of us would have were it not for the fact that we live under the demands of capital and its accumulation. We live under a situation that mis-educates and under-educates us. A situation where it’s hard for us to find out what the truth is about our society or our world. And a situation that values us the same way that miners in the 1930s were told that when the mine begins to collapse you push the mules out first because it costs money to replace a mule.That’s the position we’re in in relation to the people that hold the wealth in this world. We are expendable and they’re going to escalate that expendability. The choice and the power is there. But the choice to recognize that power, and take responsibility for it, and make this into a world where all of us can live, sits right here.
Take fiat currency: it’s money issued and backed by national governments that is not backed by physical commodities, like gold, or water, or energy. Tom Greco is a preeminent scholar, author, educator, and community economist, who, for more than 35 years has been working at the leading edge of transformational restructuring. I met Tom at a Strategies for Transforming the Global Economy conference, organized by hyper-activist Carol Brouillet in 1999, and have received his newsletters ever since. (Building the community currencies directory from 1999 to 2001 is an echo of what was collected at that time relating to work Tom was an essential mover-and-shaker in.) His 2009 book, The End of Money and the Future of Civilization “provides specific design proposals and exchange-system architectures for local, regional, national, and global financial systems, and offers strategies for their implementation prescribing actions that grassroots organizations, businesses, and governments will need to take to achieve success.” (isbn.nu and libraries)
In The Money Economy Is Not the Real Economy: “The Global Banking and Financial System is Fatally Flawed” (19 Sep 2022), Tom opens with, “Money is the ‘nothing’ that serves only to account for that which is available in the real economy; money is the ‘hole’ that is defined by the ‘doughnut’ of real goods and services. When pseudo-money can be created by fiat, apart from anything of real value, fraud, confusion, and madness ensue.”
While the past several decades have seen the emergence of many successful approaches to decentralized control of credit through private currencies and independent commercial credit clearing circles, economic and financial corporatization and globalization have overwhelmed their impact and placed ever tighter control into the hands of the elite class who have used their money power as a weapon of class warfare. The Breton Woods monetary agreement that was established toward the end of World War II made the US dollar the world’s reserve currency and allowed the US and its various allies to dominate and control the machinery of money and finance. But with the breakdown of that agreement and the increasing application of financial and economic sanctions against rivals who challenge the western unipolar world order, we now see that some countries, notably China and Russia, are taking independent action to protect their own currencies, economies, and security interests.
These countries are moving to back their currencies with real commodities as Alasdair Macleod describes in his recent article The Commodity Currency Revolution, and in this YouTube interview Commodity-Backed Currencies to Challenge Dollar Yen & Euro?. This phenomenal shift is further elucidated in other sources, including David Stockman’s Monetary Madness Among the Central Bankers, and Alastair Crooke’s post about the decline of the western financial system and the US dollar as the world reserve currency. The latter makes the point that “... the financial war on Russia gave the West an unmistakable lesson from Moscow that the hardest currencies are not USD or EUR, but rather oil, gas, wheat, and gold. Yes, energy, food and strategic resources are currencies [in the real economy].”
Another sobering thesis is being articulated by Dr. Tim Morgan at his website Surplus Energy Economics, in which he argues that, “the economy is an energy system, not a financial one,”[†] and that, “The concept of limits is replacing the paradigm of ‘infinite growth.’”[††] He rightly points out that, “What lies ahead is a process of adjustment – we might call it realignment – to the new reality of an economy in which the scope for expansion is constrained by limits, both to energy value and to environmental tolerance.”[††] Morgan’s economic model, which he calls Surplus Energy Economics Data System [SEEDS], is based on the idea that continual economic growth has been possible only through the availability of the surplus energy that comes from fossil fuels. But that surplus, which is the amount of energy obtained minus the amount of energy needed to extract it, is continuing to decline, and that fact suggests that the enormous waste of resources spent on cheap non-durable, non-repairable, and non-recyclable products and weapons of war must be phased out.
This shift toward commodity backed national currencies, while not a total solution to the money problem, is a positive step toward reconnecting the means of payment to real economic value.
This will eventually lead also to the emergence of a new standard of value against which the value of currencies, as well as goods and services, can be measured, not only against one another on foreign exchange markets, but more objectively against the value of real goods and services. That standard will not be gold, as it was in the past, but a wide assortment, or “market basket,” of useful commodities like the commodity standard I’ve been proposing for more than 40 years. History shows that, as exchange systems evolve, credit instruments become the primary payment media because the quantity of credit money is able to expand and contract in step with economic activity and the actual supplies of goods and services. Then, the selected standard commodities serve only as the measure of value and unit of account to quantify credit obligations.
Just as happened in the past with gold, I expect the commodities in a standard “basket” will serve as a new measure of value, but payments will be made using credit instruments and the credit clearing process, with perhaps, occasional settlement of residual account balances by the transfer of actual commodities. As I’ve repeatedly explained in my books and articles, it is crucial that these credit currencies be spent into circulation on the basis of an adequate real value foundation and without interest charges.
Josh Mitteldorf studies evolutionary theory of aging using computer simulations. He wrote a fascinating and compelling essay in August 2021 on What happened to Atlantis? What will happen to us? The LONG VIEW he encapsulates proffers awareness of balance and a sense of centeredness concerning the sacred nature of whatEVER is going on here. For the indescribably brief moment we wear our human overcoats, it is a constant challenge to REMEMBER, as Thelonious Monk expresses it, what we are here for. Mitteldorf concludes with how,
... the future is not yet determined, and ... we each have a hand in co-creating it. Whether the coming crisis ends our civilization or transforms it is up to us. Don’t think about “hope”, but rather pro-actively build the future we want, even before present systems collapse. My aim will be toward an end of rapacious resource exploitation, and return to local autonomy and diverse, independent human cultures.
We are privileged to live through an event as significant as the Younger Dryas extinction, but it doesn’t have to end in collapse and mass death. Let’s aim for what Charles Eisenstein calls The More Beautiful World that our Hearts Know is Possible. We must re-discover the energy source that moved 100-ton stone blocks without fossil fuels or uranium. And we must re-learn what Native American tribes knew about managing robust ecosystems enriched in foods and herbs, so that nature provides all our needs in a sustainable way that is actually more efficient even than organic agriculture.
We will have help from disembodied spirits and/or extraterrestrials.
I was blessed to work with John William Gofman, M.D., Ph.D. in the latter part of his life, publishing online copy of his decades-long research and analysis concerning the consequences of exposure to ionizing radiation. I first learned of him reading the 1982 book, Nuclear Witnesses: Insiders Speak Out. The book’s author, Leslie Freeman explained, “It is the premise of this book that if the American people knew the truth about radiation there would be no nuclear issue.” Today, if the people in the US knew the truth about the nature and consequences of SARS-CoV-2 virus and the effective early treatment protocols, there would be no “C19 Pandemic”. This is where the need to educate oneself and others one can reach is so vital, critical, and life-affirming.
John Gofman received the Right Livelihood Award in 1992 “For his pioneering work in exposing the health effects of low-level radiation.” The tenacity and fearlessness with which Gofman, and his colleague Arthur R. Tamplin, Ph.D., challenged the deceptions and falsehoods of the nuclear power industry resulted in the book, Poisoned Power, The Case Against Nuclear Power Plants Before and After Three Mile Island. By 1982, Gofman was very clear about what he saw as the necessity of reorganizing society. From his interview in Nuclear Witnesses:
Even if you made an agreement to abolish all nuclear weapons, but you left established power structure in the US and the USSR, they’d go on to research mind control or some chemical or biological thing. My view is, there exists a group of people in the world that have a disease. I call it the “power disease.” They want to rule and control other people. They are a more important plague than cancer, pneumonia, bubonic plague, tuberculosis, and heart disease put together. They can only think how to obliterate, control, and use each other. They use people as nothing more than instruments to cast aside when they don’t need them any more. There are fifty million people a year being consumed in a nutritional holocaust around the world; nobody gives a damn about starvation. If fifty million white Westerners were dying, affluent Western society would worry, but as long as it’s fifty million Third World people dying every year, it doesn’t matter.
In my opinion, what we need is to move toward being nauseated by people who want to be at the top, in power. Can you think of anything more ridiculous than that the Chinese, Russian, and American people let their governments play with superlethal toys and subject all of us to these hazards? The solution is not to replace one leader with another or to have more government. Society has to reorganize itself. The structure we have now is, the sicker you are socially, the more likely it is that you’ll come out at the top of the heap.
Speaking from his own experience 40 years ago, Gofman’s assessment is today being played out with the “biological thing”—Brought To You By.... mind control—coming home to roost.
Another illuminated soul I was blessed to know was Richard Grossman. Ralph Nader called him “the preeminent historian of corporations”. I met Richard in 1996. Inspiration from his work on the history of the corporation, and his generosity in sharing many sources of his writing, resulted in Ending Corporate Governance. Like John Gofman, Richard exercised his wide-ranging intelligence with clarity and coherence. Grossman’s 2001, How Long Shall We Grovel? Memo for the Record, dissects Bill Moyers’ PBS program, “Trade Secrets.” It is representative of his stellar critical analysis faculties. In the following replace “chemical corporations” with “biotechnology corporations” to apprehend how, in Santayana’ words, we still “cannot remember the past [and] are [being] condemned to repeat it” a thousand-fold. Grossman begins by quoting Moyers:
“We have trusted the chemical industry and our government to test the chemicals' effects on health and safety, and to take dangerous ones off the market.”Why? Based on what evidence?
The point of the Moyers’ program was that chemical corporation officials made investment, technology, sales, and promotion decisions to drench their workers and the world with what they knew were poisons, and they didn’t come clean. Commenting on the program, The New York Times Corporation said that nothing good comes without a price. The remedies suggested in Moyers’ program: passing laws that give people the “right to know” what’s in all products, and requiring the testing of chemicals before they are mass produced.
So I asked myself: Did Bill Moyers instruct his staff to discover what was known in the 1950s and 1960s and 1970s and 1980s—or earlier—about chemical corporations and poisoning? To find out what people back then were saying and doing? I took a look at my bookshelves and files.
- These excerpts show that diverse people and civic groups—along with eloquent scientists and even some elected officials—had a different vision of how to build a prosperous, productive, healthy and just society.
- They show people committed to democracy, human rights and living in harmony with the earth’s natural systems.
- They show people organizing to stop corporate and government assaults on human rights, justice and the earth’s natural systems.
- They show poisoned people demanding not vengeance but acknowledgment as human beings . . . and then, health care, reparations, justice and sanity.
- They show poisoned people educating themselves, neighbors, public officials and the nation about science, medicine, business, oppression and self-governance.
In 2001, ANYONE who chooses to look will find massive evidence of chemical corporation murder, pillage and lies extending over a century. ANYONE who chooses to look will see persistent corporate denial of people’s constitutional and human rights, and government complicity. This country exalts the platitude “all political authority is inherent in the people.” But our great corporations have long been protected by the rule of law ... empowered by our own constitution and bill of rights.
Our society has bestowed upon Chemical corporation leaders, as upon top officials of all giant corporations, the highest rewards and honors, and great wealth. Great corporations have been exalted by legislators and judges, presidents and governors, police and national guards, by local, state and federal governments.
How long shall we authorize chemical corporate officials to kill? How long shall we beg them to tell the truth? To make the earth’s air, water and soil, our foods and our jobs, a little less deadly? To please “give us” the right to know?
How long shall we grovel before our elected public servants?
Other species are counting on us to do more than regulate the destruction of the planet.
What do YOU think we the people should do now?
Richard passed over to the spirit world on 22 Nov 2011. His final work in progress was An Act To Criminalize Chartered, Incorporated Business Entities. His cogent summation of the massive evidence of chemical corporation murder, pillage and lies extending over a century, is today reaching its apex in biotechnology corporation murder, pillaging and lies. The question remains for each of us to answer: What do YOU think we the people should do now?
Concerning C19 vaccine damage, the Demands listed from the 14 Nov 2022 Media Conference as part of the Criminal Complaint against Swissmedic, are applicable globally:
I first learned of Howard Steen in the Corona Committee, Session 81, Open Your Eyes And Advance. He and colleague Karolus are on fire producing vital, life-affirming works-in-progress at: Corona Cases - The Law vs The New Normal and ShortXXvids - Documenting the New Normal, with the supporting CreativeWorks video channel. It was through Howard’s twitter channel that I first learned of the Swissmedic Criminal Complaint. Mr. Steen is an exemplar of expressing devotion and commitment to honoring and serving Life’s needs on Mother Earth. Along with so many others cited above, he is a change agent providing sacred inspiration of what occurs when one engages with one’s Creator and throws off the shackles of the deeply corrupted political and economic spheres of the world we find ourselves alive in.
Bob Moran is another of the many, many souls today, actively living out their birthright wisdom and intelligence on behalf of our single, iridescent human family. His artwork is presented throughout this essay with great appreciation for his incisive understanding of what the nature of being human means. Exercising his creativity and intelligence with clarity and coherence, he explores his conscience, rendering a wide range of distillations of our mad, mad, mad, mad, world. BoB - Brilliantly Difficult is a new film that explores the wonderful spirit of Bob Moran.

I find illumination and inspiration in the wisdom of Original Free Peoples as explored in 2018: Losing Earth? Realign with Original Free Peoples’ Great Law and Find Her Again. As well, inspiration and creative imagination is expressed by the likes of dear friend Elisabet Sahtouris in Main Features or Principles of Healthy Living Systems from cells to organisms, ecosystems to Earth, bodies to businesses. In addition, her observation about leadership in The Big Picture (1999) is clear and incisive:
Janine Benyus, author of a wonderful book called Biomimicry, pointed out that humans assigned one group of people called biologists to study how other species make a living, while a totally separate group of people called economists were to figure out how humans make a living. Now we have the opportunity to look at economics in terms of biology—to look at the experience of four-and-half billion years of self-organization, to see how young species are acquisitive and territorial and grabby, and mature species co-operate, as in a rainforest. Where is the leadership? Distributed leadership. Everything shared and recycled. What a great economic model!
So many areas of focus are needed to creatively and effectively respond to the current situation confronting all of us. The above only scratches the surface of what is needed and what can be done. Every person alive on Mother Earth has extraordinary gifts and powers to meet the challenges our species collectively faces. Once the numbing mind-fog spell is dissolved, there is no limit to what can be imagined and acted upon to contribute to discovering unknown possibilities of manifesting life-affirming processes that meet the needs of all.
|
“
|
Each individual human being is given intelligence to participate in this life
with. Before we go around blaming we should take responsibility individually,
which helps it to happen collectively, we should take responsibility to
respect our intelligence, to think as clearly and coherently as we can. And
this will start to change the energy shift because being free is about
responsibility.
Having someone to blame turns into a convenience. If we’re
not taking responsibility to use our intelligence clearly and coherently we’re
not in a position to be blaming anybody for anything. We’re not fulfilling our
end of the deal. We use it as a convenience to have someone to blame so that
we don’t have to respect our own intelligence. And if we don’t respect our
intelligence we don’t respect ourselves. And if we don’t respect our
intelligence and we don’t respect ourselves then obviously we don’t really
respect the Creator. But it’s not because we don’t want to, it’s because we
don’t know how to. And the reason we don’t know how to is because we’re not
using our intelligence clearly and coherently.
|
|
—John Trudell, Mongrel Patriot Review, Newtopia Magazine, 14 Dec 2011
|
|
It was Elisabet who introduced me to two wonder full books: Amazon Beaming and Kinship With All Life. Both books transcend and exceed the boundaries of rational thought and offer reconnection with the wisdom of our ancestors. In Kinship, at the close of the chapter titled Naked Ponies, the author shares the consciousness and conscience of the Indian Chief he had the privilege of beginning to know.
Whenever the chief met an animal or any other living thing, he would pause and establish mental contact with it. While the physical part of the chief walked the earth, the mental and spiritual part of him moved in boundless space, embracing all creation in a comprehensive kinship in which all things were important and all things needed in the divine Plan and Purpose. Ever helping him to understand and move in rhythm with all creation was his companion, counselor, guide and helper—The Big Holy.The chief never reads books, magazines or newspapers; he never listens to the radio and never watches television. Whenever he wants to know the latest news, whenever he needs fresh wisdom, mental diversion, spiritual nourishment, or clearer vision about some particular problem, he goes to what he calls the Great Library; other people call it the universe. The “Volumes” he consults in this Library are the sun, the moon, the stars, the clouds, growing things, his favorite pony, and all sorts of other animate and inanimate things. He consults them with humility, receptivity and deep reverence. His rich life experience has taught him that the Author speaking through each one of these living manuscripts is The Big Holy.
Each of us is answerable to our Creator. Each of us has an immutable relationship with the source of our existence. The ineffable mystery we each embody is eternally framed in the wonder of whatever is really going on here. John Trudell touched the essence of this in What It Means To Be A Human Being.
... because ... we come from where we come from, every one of us is the descendant of a tribe. Every person in this room is a descendant of a tribe at some point in our ancestral evolution. Common, collective, genetic memory that’s in there, you know, that’s encoded, like I say, in the DNA. And for every individual, encoded in our individual DNA, alright?, is the experience of our lineage from the very beginning. Whose whole perceptional reality was what I was just saying: all things have being, we’re made up of the Earth – all my relations, pray to spirits. See, and they didn’t pray to man or human form. The closest they came to it was they prayed to spirits that were called ancestors.Alright? And because they were praying to those ancestors for help and guidance, they understood that we were borrowing today from the past and the future. We’re borrowing it from both places. So they had this understanding of reality.... they knew that to keep the balance was the purpose.... The reason for being was to keep the balance. ... this was ... what I will call a spiritual perception of reality. And so because of the spiritual perception of reality they understood that life was about responsibility. It wasn’t about the abstraction of freedom – it was about responsibility. That life was about responsibility.
There is a vital need to activate remembering that we are borrowing today from the past as well as the future. So much forgetting makes possible the incoherent, life-destroying processes and activities that beset the world. This started a long time ago. John Trudell expresses his understanding of how, within the techno-logic perceptional reality, one of the civilizing processes is to erase memories; memory of who we are and what we are, memory of identity and self-reality.
Our single human family is dealing with the consequences of medical nemesis writ large. Ivan Illich wrote of clinical, social, and cultural iatrogenesis as being self-reinforcing: “Iatrogenesis is clinical when pain, sickness, and death result from medical care; it is social when health policies reinforce an industrial organization that generates ill-health; it is cultural and symbolic when medically sponsored behavior and delusions restrict the vital autonomy of people by undermining their competence in growing up, caring for each other, and aging, or when medical intervention cripples personal responses to pain, disability, impairment, anguish, and death.” Today, the Domination System’s imperative to permanently extinguish our vital autonomy is reaching critical mass. The immutable bond and individual relationship to the Big Holy each of us was born with is the eternal source of balance and strength guiding and informing our steps.
Fighting back today is an all-or-nothing struggle. Children and all those yet unborn look to us for the sake and integrity of their future; a life-affirming and life-loving future where humility, receptivity, compassion and empathy, and deep reverence inform all choices made on behalf of the seventh generation yet unborn. The close of the Introduction to Marty Schotz’s 1996 book brings us full circle to the challenge all of us who honor our Creator are summoned to be informed by.
As citizens who have turned away for thirty years from the truth of the murder of our elected head of state, we should not be surprised that today we find our nation in intellectual, political, and moral chaos. Confronting the truth of President Kennedy’s assassination and its coverup is but one small step on a long path out of that chaos and toward healing, a path along which we must confront the true nature of our democracy and the reality of what our nation has become for its own citizens and for people throughout the world. Such a process of healing is not pleasant. It is a difficult and painful path, but it is a necessary one. History will not absolve us.
The GOOD NEWS is the expanding mass of souls devoted to honoring and serving Life’s needs here on Mother Earth. Just now discovering Sasha Latypova’s re-ignited substack. Her Be Not Afraid: Introduction, My Background and Motivation acknowledges the silver lining to the Domination System’s spawn including the US military prototype project:
I collaborate with 100+ amazing people whom I met in this fight - scientists, doctors, engineers, software wizards, lawyers, journalists. As many will attest, the silver lining of the global descent into totalitarian hell is that we met each other. Working with these incredible individuals fills me with a profound sense of awe in the divine power that created and guides us, gives me (maybe irrational) sense of optimism, and motivates me to do more.
See Appendix 14 for some of the souls giving their all to support our single, fragile, supremely gifted human family. Annnd, those cited/referenced above in this essay, are but a very, very small number of people confronting the true nature of our society, what our nation has become for its own citizens and for people throughout the world, and committed to lay bare the darkness and promote the light.
|
“
|
It’s that everything [in the Cold War in 1962-1963] was totally out of control and then, through a kind of incredible process where these two men were communicating secretly with each other over the year previous [Sep 1962-63], and smuggling letters back and forth to each other, in the midst of this conflict, they were beginning to trust each other.... It’s a remarkable process. And it’s all beneath the surface. But so are all the things that count as Merton understood.... And that’s why I have some hopes that if we are willing to go deeply enough into the darkness – and Kennedy was, and Khrushchev was – anything can happen for the good. But if we don’t go into the darkness it doesn’t happen.
—Jim Douglass at Elliot Bay Books, 6 May 6, 2008
|
“Even if I were pollinated and fully vaccinated, I would admire the unvaccinated for withstanding the greatest pressure I have ever seen, even from partners, parents, children, friends, colleagues and doctors.
People who were capable of such personality, courage and critical ability are undoubtedly the best of humanity. They are everywhere, in all ages, levels of education, states and ideas. They are of a special kind; they are the soldiers that every army of light wants to have in its ranks. They are the parents that every child wants to have and the children that every parent dreams of having. They are beings above the average of their societies, they are the essence of the people who have built all cultures and conquered horizons. They are there, next to you, they look normal, but they are superheroes.
They did what others could not, they were the tree that withstood the hurricane of insults, discrimination and social exclusion. And they did it because they thought they were alone, and believed they were the only ones.
Banned from their families’ tables at Christmas, they never saw anything so cruel. They lost their jobs, let their careers sink, had no more money ... but they didn’t care. They suffered immeasurable discrimination, denunciation, betrayal and humiliation ... but they kept going.
Never before in humanity has there been such a ‘casting’, now we know who are the best on planet Earth. Women, men, old, young, rich, poor, of all races or religions, the unvaccinated, the chosen of the invisible ark, the only ones who managed to resist when everything collapsed. That’s you, you passed an unimaginable test that many of the toughest Marines, Commandos, Green Berets, astronauts and geniuses could not withstand.
You are made of the stuff of the greatest who ever lived, those heroes born among ordinary men who glow in the dark.”
As of 7 April 2023, the US Vaccine Adverse Events Reporting System (VAERS) has logged 2,458,057 COVID Vaccine Adverse Event Reports. Established in 1990, VAERS is a voluntary reporting system that has been estimated to account for only 1% of vaccine injuries (see page 6 of the Lazarus Report). For 7 April 2023, the system recorded 35,096 COVID Vaccine Reported Deaths.
Given that a small percentage of genuine vaccine injuries—including death—are recorded in VAERS, the actual lethality of these injections begs a number of beyond-hideous questions. Why is there no reporting on this? Why is this not page-1 banner headlines on every newspaper and news program every day? Why has the FDA continued to approve more and more shots, especially for healthy younger and middle-aged adults and children? Why has Covid Czar Ashish Jha continued to say these injections are safe and effective?
A breakdown of the VAERS data is listed in the OpenVAERS Project, allowing browsing and searching of reports without needing to compose advanced searches:
|

“Reaction Group” fatalities chart

“The European Medicines Agency publishes these data so that its stakeholders, including the general public, can access information that European regulatory authorities use to review the safety of a medicine or active substance. Transparency is a key guiding principle of the Agency.”
In October 2020, COVID-19 Data Collection, Comorbidity & Federal Law: A Historical Retrospective was published in the journal Public Health Policy Initiative by the Institute for Pure and Applied Knowledge.
In March of 2021, the COVID research team took the liberty of collecting, organizing, and publishing hundreds of references in this wide-ranging, peer-reviewed magnum opus, COVID-19: Restoring Public Trust During A Health Crisis. The peer-reviewed scientific literature and clinical evidence overwhelmingly demonstrates that asymptomatic transmission is a failed theory, PCR testing is fatally flawed, evidence-based treatments exist, projection models have been massively inaccurate, clinical trials for the experimental biologics have not demonstrated safety or effectiveness, and that the greatest freedoms under assault are compassion, love, and moral courage in medicine.
In June of 2021, the Santa Clara County California public health department performed a partial audit of death certificate records where COVID was listed as the cause of death and found that the data was hyper-inflated by 22%.
In July of 2021, the Alameda County California public health department performed a partial audit of death certificate records where COVID was listed as the cause of death and found that the data was hyper-inflated by 25%.
Partial audits of death certificates entail removing obvious reporting inaccuracies such as car accidents, physical accidents, etc. being counted as COVID caused deaths.
Full audits of death certificates, which my research team has been calling for since October of 2020, entail a review of full medical records, including any autopsy results, so the cause of death can be definitively confirmed.
Santa Clara County and Alameda County California are large population centers and prove our point that the changes adopted by the CDC in violation of federal law led to inaccurate data that significantly hyper-inflated case, hospitalization, and death counts. To make matters worse, these inaccuracies were rewarded with a higher Medicare/Medicaid reimbursement and no consequences as yet for the massive errors that have compromised all published COVID data.

The image above displays 5 columns of COVID data published through February 6, 2022.
Looking left to right, column one displays that COVID death count published by the CDC. This is the total number of deaths published using the March 24th, 2020 COVID Alert No. 2.
The 2nd column displays a projected value assuming that soft audits of all death certificates would be similar to what occurred in Santa Clara & Alameda Counties and produce a 25% reduction in death counts.
The middle column displays the projected maximum reduction in death counts if a full audit of all records was based upon the 2003 death certificate reporting handbooks published by the CDC and still in use for all causes of death except COVID. It is important to note that the CDC states as of February 6, 2022 that, “For over 5% of these deaths, COVID-19 was the only cause mentioned on the death certificate. For deaths with conditions or causes in addition to COVID-19, on average, there were 4.0 additional conditions or causes per death.” This statement has remained unchanged since at least July 2021.
The 4th column is the total number of deaths reported to the Vaccine Adverse Events Reporting System (VAERS) as of February 4, 2022.
The 5th column is the estimated number of actual deaths based upon the case filing filed by attorney Tom Renz in the US District Court of Alabama on July 19, 2021, which asserts under penalty of perjury that data being reported to VAERS is significantly under reported by a factor of 5 at the very minimum.
Collectively, this graphic contends that a full audit of all COVID death certificates could reveal that more people have died in connection with the experimental COVID inoculations than due to complications from the SARS-CoV-2 infection had federal laws not been violated, hyper-inflating COVID data published by the CDC.
Above are the lower-limit reports of injuries and deaths. Concerning the upper limit estimate of deaths caused by the C19 “Vaccines”:
Experts estimate 20 million are already dead due to COVID Vaccination & over 2 billion injured, The Exposé, 1 Oct 2022
as described by Dr. Roger Hodkinson here:
20 Million Dead from the Jab, 2.2 Billion Injuries – Analyst Estimates.
Complete film is here: Laura-Lynn Tyler Thompson
with Dr. Roger Hodkinson; Fertility, Cancer, Flight Safety and SADS, 5 Oct 2022
Until Proven Otherwise - Two Cardiologists Expose Big Pharma, Justus R. Hope, Repurposed Drugs: Powers & Possibilities, 19 Dec 2022
“Until Proven Otherwise” Two World Renowned Cardiologists independently reach the same medical conclusions. US American Peter McCullough, MD, MPH, and British Aseem Malhotra, MD state that their medical opinion is that the sudden deaths, especially in young people, are caused by the Covid-19 mRNA vaccines, until proven otherwise. Nov 2022
In order of appearance:
This is a miniscule portion of what the United States Food and Drug Administration of the United States Executive Branch of the United States Federal Government tried—and failed—to lock away from the WE THE PEOPLE and deny access to for SEVENTY-FIVE YEARS. Pages 30-38 lists 1,284 adverse events in 5.3.6 CUMULATIVE ANALYSIS OF POST-AUTHORIZATION ADVERSE EVENT REPORTS OF PF-07302048 (BNT162B2) RECEIVED THROUGH 28-FEB-2021
APPENDIX 1. LIST OF ADVERSE EVENTS OF SPECIAL INTEREST
lp36 deletion syndrome
2-Hydroxyglutaric aciduria
5'nucleotidase increased
Acoustic neuritis
Acquired Cl inhibitor deficiency
Acquired epidermolysis bullosa
Acquired epileptic aphasia
Acute cutaneous lupus erythematosus
Acute disseminated encephalomyelitis
Acute encephalitis with refractory, repetitive partial seizures
Acute febrile neutrophilic dermatosis
Acute flaccid myelitis
Acute haemorrhagic leukoencephalitis
Acute haemorrhagic oedema of infancy
Acute kidney injury
Acute macular outer retinopathy
Acute motor axonal neuropathy
Acute motor-sensory axonal neuropathy
Acute myocardial infarction
Acute respiratory distress syndrome
Acute respiratory failure
Addison's disease
Administration site thrombosis
Administration site vasculitis
Adrenal thrombosis
Adverse event following immunisation
Ageusia
Agranulocytosis
Air embolism
Alanine aminotransferase abnormal
Alanine aminotransferase increased
Alcoholic seizure
Allergic bronchopulmonary mycosis
Allergic oedema
Alloimmune hepatitis
Alopecia areata
Alpers disease
Alveolar proteinosis
Ammonia abnormal
Ammonia increased
Amniotic cavity infection
Amygdalohippocampectomy
Amyloid arthropathy
Amyloidosis
Amyloidosis senile
Anaphylactic reaction
Anaphylactic shock
Anaphylactic transfusion reaction
Anaphylactoid reaction
Anaphylactoid shock
Anaphylactoid syndrome of pregnancy
Angioedema
Angiopathic neuropathy
Ankylosing spondylitis
Anosmia
Antiacetylcholine receptor antibody positive
Anti-actin antibody positive
Anti-aquaporin-4 antibody positive
Anti-basal ganglia antibody positive
Anti-cyclic citrullinated peptide antibody positive
Anti-epithelial antibody positive
Anti-erythrocyte antibody positive
Anti-exosome complex antibody positive
Anti-GAD antibody negative
Anti-GAD antibody positive
Anti-ganglioside antibody positive
Antigliadin antibody positive
Anti-glomerular basement membrane antibody positive
Anti-glomerular basement membrane disease
Anti-glycyl-tRNA synthetase antibody positive
Anti-HLA antibody test positive
Anti-IA2 antibody positive
Anti-insulin antibody increased
Anti-insulin antibody positive
Anti-insulin receptor antibody increased
Anti-insulin receptor antibody positive
Anti-interferon antibody negative
Anti-interferon antibody positive
Anti-islet cell antibody positive
Antimitochondrial antibody positive
Anti-muscle specific kinase antibody positive
Anti-myelin-associated glycoprotein antibodies positive
Anti-myelin-associated glycoprotein associated polyneuropathy
Antimyocardial antibody positive
Anti-neuronal antibody positive
Antineutrophil cytoplasmic antibody increased
Antineutrophil cytoplasmic antibody positive
Anti-neutrophil cytoplasmic antibody positive vasculitis
Anti-NMDA antibody positive
Antinuclear antibody increased
Antinuclear antibody positive
Antiphospholipid antibodies positive
Antiphospholipid syndrome
Anti-platelet antibody positive
Anti-prothrombin antibody positive
Antiribosomal P antibody positive
Anti-RNA polymerase III antibody positive
Anti-saccharomyces cerevisiae antibody test positive
Anti-sperm antibody positive
Anti-SRP antibody positive
Antisynthetase syndrome
Anti-thyroid antibody positive
Anti-transglutaminase antibody increased
Anti-VGCC antibody positive
Anti-VGKC antibody positive
Anti-vimentin antibody positive
Antiviral prophylaxis
Antiviral treatment
Anti-zinc transporter 8 antibody positive
Aortic embolus
Aortic thrombosis
Aortitis
Aplasia pure red cell
Aplastic anaemia
Application site thrombosis
Application site vasculitis
Arrhythmia
Arterial bypass occlusion
Arterial bypass thrombosis
Arterial thrombosis
Arteriovenous fistula thrombosis
Arteriovenous graft site stenosis
Arteriovenous graft thrombosis
Arteritis
Arteritis coronary
Arthralgia
Arthritis
Arthritis enteropathic
Ascites
Aseptic cavernous sinus thrombosis
Aspartate aminotransferase abnormal
Aspartate aminotransferase increased
Aspartate-glutamate-transporter deficiency
AST to platelet ratio index increased
AST/ALT ratio abnormal
Asthma
Asymptomatic COYID-19
Ataxia
Atheroembolism
Atonic seizures
Atrial thrombosis
Atrophic thyroiditis
Atypical benign partial epilepsy
Atypical pneumonia
Aura
Autoantibody positive
Autoimmune anaemia
Autoimmune aplastic anaemia
Autoimmune arthritis
Autoimmune blistering disease
Autoimmune cholangitis
Autoimmune colitis
Autoimmune demyelinating disease
Autoimmune dermatitis
Autoimmune disorder
Autoimmune encephalopathy
Autoimmune endocrine disorder
Autoimmune enteropathy
Autoimmune eye disorder
Autoimmune haemolytic anaemia
Autoimmune heparin-induced thrombocytopenia
Autoimmune hepatitis
Autoimmune hyperlipidaemia
Autoimmune hypothyroidism
Autoimmune inner ear disease
Autoimmune lung disease
Autoimmune lymphoproliferative syndrome
Autoimmune myocarditis
Autoimmune myositis
Autoimmune nephritis
Autoimmune neuropathy
Autoimmune neutropenia
Autoimmune pancreatitis
Autoimmune pancytopenia
Autoimmune pericarditis
Autoimmune retinopathy
Autoimmune thyroid disorder
Autoimmune thyroiditis
Autoimmune uveitis
Autoinflammation with infantile enterocolitis
Autoinflammatory disease
Automatism epileptic
Autonomic nervous system imbalance
Autonomic seizure
Axial spondyloarthritis
Axillary vein thrombosis
Axonal and demyelinating polyneuropathy
Axonal neuropathy
Bacterascites
Baltic myoclonic epilepsy
Band sensation
Basedow's disease
Basilar artery thrombosis
Basophilopenia
B-cell aplasia
Behcet's syndrome
Benign ethnic neutropenia
Benign familial neonatal convulsions
Benign familial pemphigus
Benign rolandic epilepsy
Beta-2 glycoprotein antibody positive
Bickerstaffs encephalitis
Bile output abnormal
Bile output decreased
Biliary ascites
Bilirubin conjugated abnormal
Bilirubin conjugated increased
Bilirubin urine present
Biopsy liver abnormal
Biotinidase deficiency
Birdshot chorioretinopathy
Blood alkaline phosphatase abnormal
Blood alkaline phosphatase increased
Blood bilirubin abnormal
Blood bilirubin increased
Blood bilirubin unconjugated increased
Blood cholinesterase abnormal
Blood cholinesterase decreased
Blood pressure decreased
Blood pressure diastolic decreased
Blood pressure systolic decreased
Blue toe syndrome
Brachiocephalic vein thrombosis
Brain stem embolism
Brain stem thrombosis
Bromosulphthalein test abnormal
Bronchial oedema
Bronchitis
Bronchitis mycoplasmal
Bronchitis viral
Bronchopulmonary aspergillosis allergic
Bronchospasm
Budd-Chiari syndrome
Bulbar palsy
Butterfly rash
Clq nephropathy
Caesarean section
Calcium embolism
Capillaritis
Caplan's syndrome
Cardiac amyloidosis
Cardiac arrest
Cardiac failure
Cardiac failure acute
Cardiac sarcoidosis
Cardiac ventricular thrombosis
Cardiogenic shock
Cardiolipin antibody positive
Cardiopulmonary failure
Cardio-respiratory arrest
Cardio-respiratory distress
Cardiovascular insufficiency
Carotid arterial embolus
Carotid artery thrombosis
Cataplexy
Catheter site thrombosis
Catheter site vasculitis
Cavernous sinus thrombosis
CDKL5 deficiency disorder
CEC syndrome
Cement embolism
Central nervous system lupus
Central nervous system vasculitis
Cerebellar artery thrombosis
Cerebellar embolism
Cerebral amyloid angiopathy
Cerebral arteritis
Cerebral artery embolism
Cerebral artery thrombosis
Cerebral gas embolism
Cerebral microembolism
Cerebral septic infarct
Cerebral thrombosis
Cerebral venous sinus thrombosis
Cerebral venous thrombosis
Cerebrospinal thrombotic tamponade
Cerebrovascular accident
Change in seizure presentation
Chest discomfort
Child-Pugh-Turcotte score abnormal
Child-Pugh-Turcotte score increased
Chillblains
Choking
Choking sensation
Cholangitis sclerosing
Chronic autoimmune glomerulonephritis
Chronic cutaneous lupus erythematosus
Chronic fatigue syndrome
Chronic gastritis
Chronic inflammatory demyelinating polyradiculoneuropathy
Chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids
Chronic recurrent multifocal osteomyelitis
Chronic respiratory failure
Chronic spontaneous urticaria
Circulatory collapse
Circumoral oedema
Circumoral swelling
Clinically isolated syndrome
Clonic convulsion
Coeliac disease
Cogan's syndrome
Cold agglutinins positive
Cold type haemolytic anaemia
Colitis
Colitis erosive
Colitis herpes
Colitis microscopic
Colitis ulcerative
Collagen disorder
Collagen-vascular disease
Complement factor abnormal
Complement factor Cl decreased
Complement factor C2 decreased
Complement factor C3 decreased
Complement factor C4 decreased
Complement factor decreased
Computerised tomogram liver abnormal
Concentric sclerosis
Congenital anomaly
Congenital bilateral perisylvian syndrome
Congenital herpes simplex infection
Congenital myasthenic syndrome
Congenital varicella infection
Congestive hepatopathy
Convulsion in childhood
Convulsions local
Convulsive threshold lowered
Coombs positive haemolytic anaemia
Coronary artery disease
Coronary artery embolism
Coronary artery thrombosis
Coronary bypass thrombosis
Coronavirus infection
Coronavirus test
Coronavirus test negative
Coronavirus test positive
Corpus callosotomy
Cough
Cough variant asthma
COVID-19
COVID-19 immunisation
COVID-19 pneumonia
COYID-19 prophylaxis
COYID-19 treatment
Cranial nerve disorder
Cranial nerve palsies multiple
Cranial nerve paralysis
CREST syndrome
Crohn's disease
Cryofibrinogenaemia
Cryoglobulinaemia
CSF oligoclonal band present
CSWS syndrome
Cutaneous amyloidosis
Cutaneous lupus erythematosus
Cutaneous sarcoidosis
Cutaneous vasculitis
Cyanosis
Cyclic neutropenia
Cystitis interstitial
Cytokine release syndrome
Cytokine storm
De novo purine synthesis inhibitors associated acute inflammatory syndrome
Death neonatal
Deep vein thrombosis
Deep vein thrombosis postoperative
Deficiency of bile secretion
Deja vu
Demyelinating polyneuropathy
Demyelination
Dermatitis
Dermatitis bullous
Dermatitis herpetiformis
Dermatomyositis
Device embolisation
Device related thrombosis
Diabetes mellitus
Diabetic ketoacidosis
Diabetic mastopathy
Dialysis amyloidosis
Dialysis membrane reaction
Diastolic hypotension
Diffuse vasculitis
Digital pitting scar
Disseminated intravascular coagulation
Disseminated intravascular coagulation in newborn
Disseminated neonatal herpes simplex
Disseminated varicella
Disseminated varicella zoster vaccine virus infection
Disseminated varicella zoster virus infection
DNA antibody positive
Double cortex syndrome
Double stranded DNA antibody positive
Dreamy state
Dressler's syndrome
Drop attacks
Drug withdrawal convulsions
Dyspnoea
Early infantile epileptic encephalopathy with burst-suppression
Eclampsia
Eczema herpeticum
Embolia cutis medicamentosa
Embolic cerebellar infarction
Embolic cerebral infarction
Embolic pneumonia
Embolic stroke
Embolism
Embolism arterial
Embolism venous
Encephalitis
Encephalitis allergic
Encephalitis autoimmune
Encephalitis brain stem
Encephalitis haemorrhagic
Encephalitis periaxialis diffusa
Encephalitis post immunisation
Encephalomyelitis
Encephalopathy
Endocrine disorder
Endocrine ophthalmopathy
Endotracheal intubation
Enteritis
Enteritis leukopenic
Enterobacter fasciitis
Eosinophilic granulomatosis with polyangiitis
Eosinophilic oesophagitis
Epidermolysis
Epilepsy
Epilepsy surgery
Epilepsy with myoclonic-atonic seizures
Epileptic aura
Epileptic psychosis
Erythema
Erythema induratum
Erythema multiforme
Erythema nodosum
Evans syndrome
Exanthema subitum
Expanded disability status scale score decreased
Expanded disability status scale score increased
Exposure to communicable disease
Exposure to SARS-CoY-2
Eye oedema
Eye pruritus
Eye swelling
Eyelid oedema
Face oedema
Facial paralysis
Facial paresis
Faciobrachial dystonic seizure
Fat embolism
Febrile convulsion
Febrile infection-related epilepsy syndrome
Febrile neutropenia
Felty's syndrome
Femoral artery embolism
Fibrillary glomerulonephritis
Fibromyalgia
Flushing
Foaming at mouth
Focal cortical resection
Focal dyscognitive seizures
Foetal distress syndrome
Foetal placental thrombosis
Foetor hepaticus
Foreign body embolism
Frontal lobe epilepsy
Fulminant type 1 diabetes mellitus
Galactose elimination capacity test abnormal
Galactose elimination capacity test decreased
Gamma-glutamyltransferase abnormal
Gamma-glutamyltransferase increased
Gastritis herpes
Gastrointestinal amyloidosis
Gelastic seizure generalised onset non-motor seizure
Generalised tonic-clonic seizure
Genital herpes
Genital herpes simplex
Genital herpes zoster
Giant cell arteritis
Glomerulonephritis
Glomerulonephritis membranoproliferative
Glomerulonephritis membranous
Glomerulonephritis rapidly progressive
Glossopharyngeal nerve paralysis
Glucose transporter type 1 deficiency syndrome
Glutamate dehydrogenase increased
Glycocholic acid increased
GM2 gangliosidosis
Goodpasture's syndrome
Graft thrombosis
Granulocytopenia
Granulocytopenia neonatal
Granulomatosis with polyangiitis
Granulomatous dermatitis
Grey matter heterotopia
Guanase increased
Guillain-Barre syndrome
Haemolytic anaemia
Haemophagocytic lymphohistiocytosis
Haemorrhage
Haemorrhagic ascites
Haemorrhagic disorder
Haemorrhagic pneumonia
Haemorrhagic varicella syndrome
Haemorrhagic vasculitis
Hantavirus pulmonary infection
Hashimoto's encephalopathy
Hashitoxicosis
Hemimegalencephaly
Henoch-Schonlein purpura
Henoch-Schonlein purpura nephritis
Hepaplastin abnormal
Hepaplastin decreased
Heparin-induced thrombocytopenia
Hepatic amyloidosis
Hepatic artery embolism
Hepatic artery flow decreased
Hepatic artery thrombosis
Hepatic enzyme abnormal
Hepatic enzyme decreased
Hepatic enzyme increased
Hepatic fibrosis marker abnormal
Hepatic fibrosis marker increased
Hepatic function abnormal
Hepatic hydrothorax
Hepatic hypertrophy
Hepatic hypoperfusion
Hepatic lymphocytic infiltration
Hepatic mass
Hepatic pain
Hepatic sequestration
Hepatic vascular resistance increased
Hepatic vascular thrombosis
Hepatic vein embolism
Hepatic vein thrombosis
Hepatic venous pressure gradient abnormal
Hepatic venous pressure gradient increased
Hepatitis
Hepatobiliary scan abnormal
Hepatomegaly
Hepatosplenomegaly
Hereditary angioedema with C1 esterase inhibitor deficiency
Herpes dermatitis
Herpes gestationis
Herpes oesophagitis
Herpes ophthalmic
Herpes pharyngitis
Herpes sepsis
Herpes simplex
Herpes simplex cervicitis
Herpes simplex colitis
Herpes simplex encephalitis
Herpes simplex gastritis
Herpes simplex hepatitis
Herpes simplex meningitis
Herpes simplex meningoencephalitis
Herpes simplex meningomyelitis
Herpes simplex necrotising retinopathy
Herpes simplex oesophagitis
Herpes simplex otitis extema
Herpes simplex pharyngitis
Herpes simplex pneumonia
Herpes simplex reactivation
Herpes simplex sepsis
Herpes simplex viraemia
Herpes simplex virus conjunctivitis neonatal
Herpes simplex visceral
Herpes virus infection
Herpes zoster
Herpes zoster cutaneous disseminated
Herpes zoster infection neurological
Herpes zoster meningitis
Herpes zoster meningoencephalitis
Herpes zoster meningomyelitis
Herpes zoster meningoradiculitis
Herpes zoster necrotising retinopathy
Herpes zoster oticus
Herpes zoster pharyngitis
Herpes zoster reactivation
Herpetic radiculopathy
Histone antibody positive
Hoigne's syndrome
Human herpesvirus 6 encephalitis
Human herpesvirus 6 infection
Human herpesvirus 6 infection reactivation
Human herpesvirus 7 infection
Human herpesvirus 8 infection
Hyperammonaemia
Hyperbilirubinaemia
Hypercholia
Hypergammaglobulinaemia benign monoclonal
Hyperglycaemic seizure
Hypersensitivity
Hypersensitivity vasculitis
Hyperthyroidism
Hypertransaminasaemia
Hyperventilation
Hypoalbuminaemia
Hypocalcaemic seizure
Hypogammaglobulinaemia
Hypoglossal nerve paralysis
Hypoglossal nerve paresis
Hypoglycaemic seizure
Hyponatraemic seizure
Hypotension
Hypotensive crisis
Hypothenar hammer syndrome
Hypothyroidism
Hypoxia
Idiopathic CD4 lymphocytopenia
Idiopathic generalised epilepsy
Idiopathic interstitial pneumonia
Idiopathic neutropenia
Idiopathic pulmonary fibrosis
IgA nephropathy
IgM nephropathy
IIIrd nerve paralysis
IIIrd nerve paresis
Iliac artery embolism
Immune thrombocytopenia
Immune-mediated adverse reaction
Immune-mediated cholangitis
Immune-mediated cholestasis
Immune-mediated cytopenia
Immune-mediated encephalitis
Immune-mediated encephalopathy
Immune-mediated endocrinopathy
Immune-mediated enterocolitis
Immune-mediated gastritis
Immune-mediated hepatic disorder
Immune-mediated hepatitis
Immune-mediated hyperthyroidism
Immune-mediated hypothyroidism
Immune-mediated myocarditis
Immune-mediated myositis
Immune-mediated nephritis
Immune-mediated neuropathy
Immune-mediated pancreatitis
Immune-mediated pneumonitis
Immune-mediated renal disorder
Immune-mediated thyroiditis
Immune-mediated uveitis
Immunoglobulin G4 related disease
Immunoglobulins abnormal
Implant site thrombosis
Inclusion body myositis
Infantile genetic agranulocytosis
Infantile spasms
Infected vasculitis
Infective thrombosis
Inflammation
Inflammatory bowel disease
Infusion site thrombosis
Infusion site vasculitis
Injection site thrombosis
Injection site urticaria
Injection site vasculitis
Instillation site thrombosis
Insulin autoimmune syndrome
Interstitial granulomatous dermatitis
Interstitial lung disease
Intracardiac mass
Intracardiac thrombus
Intracranial pressure increased
Intrapericardial thrombosis
Intrinsic factor antibody abnormal
Intrinsic factor antibody positive
IPEX syndrome
Irregular breathing
IRVAN syndrome
IVth nerve paralysis
IVth nerve paresis
JC polyomavirus test positive
JC virus CSF test positive
Jeavons syndrome
Jugular vein embolism
Jugular vein thrombosis
Juvenile idiopathic arthritis
Juvenile myoclonic epilepsy
Juvenile polymyositis
Juvenile psoriatic arthritis
Juvenile spondyloarthritis
Kaposi sarcoma inflammatory cytokine syndrome
Kawasaki's disease
Kayser-Fleischer ring
Keratoderma blenorrhagica
Ketosis-prone diabetes mellitus
Kounis syndrome
Lafora's myoclonic epilepsy
Lambl's excrescences
Laryngeal dyspnoea
Laryngeal oedema
Laryngeal rheumatoid arthritis
Laryngospasm
Laryngotracheal oedema
Latent autoimmune diabetes in adults
LE cells present
Lemierre syndrome
Lennox-Gastaut syndrome
Leucine aminopeptidase increased
Leukoencephalomyelitis
Leukoencephalopathy
Leukopenia
Leukopenia neonatal
Lewis-Sumner syndrome
Lhermitte's sign
Lichen planopilaris
Lichen planus
Lichen sclerosus
Limbic encephalitis
Linear IgA disease
Lip oedema
Lip swelling
Liver function test abnormal
Liver function test decreased
Liver function test increased
Liver induration
Liver injury
Liver iron concentration abnormal
Liver iron concentration increased
Liver opacity
Liver palpable
Liver sarcoidosis
Liver scan abnormal
Liver tendemess
Low birth weight baby
Lower respiratory tract herpes infection
Lower respiratory tract infection
Lower respiratory tract infection viral
Lung abscess
Lupoid hepatic cirrhosis
Lupus cystitis
Lupus encephalitis
Lupus endocarditis
Lupus enteritis
Lupus hepatitis
Lupus myocarditis
Lupus myositis
Lupus nephritis
Lupus pancreatitis
Lupus pleurisy
Lupus pneumonitis
Lupus vasculitis
Lupus-like syndrome
Lymphocytic hypophysitis
Lymphocytopenia neonatal
Lymphopenia
MAGIC syndrome
Magnetic resonance imaging liver abnormal
Magnetic resonance proton density fat fraction measurement
Mahler sign
Manufacturing laboratory analytical testing issue
Manufacturing materials issue
Manufacturing production issue
Marburg's variant multiple sclerosis
Marchiafava-Bignami disease
Marine Lenhart syndrome
Mastocytic enterocolitis
Matemal exposure during pregnancy
Medical device site thrombosis
Medical device site vasculitis
MELAS syndrome
Meningitis
Meningitis aseptic
Meningitis herpes
Meningoencephalitis herpes simplex neonatal
Meningoencephalitis herpetic
Meningomyelitis herpes
MERS-CoV test
MERS-CoV test negative
MERS-CoV test positive
Mesangioproliferative glomerulonephritis
Mesenteric artery embolism
Mesenteric artery thrombosis
Mesenteric vein thrombosis
Metapneumovirus infection
Metastatic cutaneous Crohn's disease
Metastatic pulmonary embolism
Microangiopathy
Microembolism
Microscopic polyangiitis
Middle East respiratory syndrome
Migraine-triggered seizure
Miliary pneumonia
Miller Fisher syndrome
Mitochondrial aspartate aminotransferase increased
Mixed connective tissue disease
Model for end stage liver disease score abnormal
Model for end stage liver disease score increased
Molar ratio of total branched-chain amino acid to tyrosine
Molybdenum cofactor deficiency
Monocytopenia
Mononeuritis
Mononeuropathy multiplex
Morphoea
Morvan syndrome
Mouth swelling
Moyamoya disease
Multifocal motor neuropathy
Multiple organ dysfunction syndrome
Multiple sclerosis
Multiple sclerosis relapse
Multiple sclerosis relapse prophylaxis
Multiple subpial transection
Multisystem inflammatory syndrome in children
Muscular sarcoidosis
Myasthenia gravis
Myasthenia gravis crisis
Myasthenia gravis neonatal
Myasthenic syndrome
Myelitis
Myelitis transverse
Myocardial infarction
Myocarditis
Myocarditis post infection
Myoclonic epilepsy
Myoclonic epilepsy and ragged-red fibres
Myokymia
Myositis
Narcolepsy
Nasal herpes
Nasal obstruction
Necrotising herpetic retinopathy
Neonatal Crohn's disease
Neonatal epileptic seizure
Neonatal lupus erythematosus
Neonatal mucocutaneous herpes simplex
Neonatal pneumonia
Neonatal seizure
Nephritis
Nephrogenic systemic fibrosis
Neuralgic amyotrophy
Neuritis
Neuritis cranial
Neuromyelitis optica pseudo relapse
Neuromyelitis optica spectrum disorder
Neuromyotonia
Neuronal neuropathy
Neuropathy peripheral
Neuropathy, ataxia, retinitis pigmentosa syndrome
Neuropsychiatric lupus
Neurosarcoidosis
Neutropenia
Neutropenia neonatal
Neutropenic colitis
Neutropenic infection
Neutropenic sepsis
Nodular rash
Nodular vasculitis
Noninfectious myelitis
Noninfective encephalitis
Noninfective encephalomyelitis
Noninfective oophoritis
Obstetrical pulmonary embolism
Occupational exposure to communicable disease
Occupational exposure to SARS-CoY-2
Ocular hyperaemia
Ocular myasthenia
Ocular pemphigoid
Ocular sarcoidosis
Ocular vasculitis
Oculofacial paralysis
Oedema
Oedema blister
Oedema due to hepatic disease
Oedema mouth
Oesophageal achalasia
Ophthalmic artery thrombosis
Ophthalmic herpes simplex
Ophthalmic herpes zoster
Ophthalmic vein thrombosis
Optic neuritis
Optic neuropathy
Optic perineuritis
Oral herpes
Oral lichen planus
Oropharyngeal oedema
Oropharyngeal spasm
Oropharyngeal swelling
Osmotic demyelination syndrome
Ovarian vein thrombosis
Overlap syndrome
Paediatric autoimmune neuropsychiatric disorders associated with streptococcal infection
Paget-Schroetter syndrome
Palindromic rheumatism
Palisaded neutrophilic granulomatous dermatitis
Palmoplantar keratoderma
Palpable purpura
Pancreatitis
Panencephalitis
Papillophlebitis
Paracancerous pneumonia
Paradoxical embolism
Parainfluenzae viral laryngotracheobronchitis
Paraneoplastic dermatomyositis
Paraneoplastic pemphigus
Paraneoplastic thrombosis
Paresis cranial nerve
Parietal cell antibody positive
Paroxysmal nocturnal haemoglobinuria
Partial seizures
Partial seizures with secondary generalisation
Patient isolation
Pelvic venous thrombosis
Pemphigoid
Pemphigus
Penile vein thrombosis
Pericarditis
Pericarditis lupus
Perihepatic discomfort
Periorbital oedema
Periorbital swelling peripheral artery thrombosis
Peripheral embolism
Peripheral ischaemia
Peripheral vein thrombus extension
Periportal oedema
Peritoneal fluid protein abnormal
Peritoneal fluid protein decreased
Peritoneal fluid protein increased
Peritonitis lupus
Pernicious anaemia
Petit mal epilepsy
Pharyngeal oedema
Pharyngeal swelling
Pityriasis lichenoides et varioliformis acuta
Placenta praevia
Pleuroparenchymal fibroelastosis
Pneumobilia
Pneumonia
Pneumonia adenoviral
Pneumonia cytomegaloviral
Pneumonia herpes viral
Pneumonia influenzal
Pneumonia measles
Pneumonia mycoplasmal
Pneumonia necrotising
Pneumonia parainfluenzae viral
Pneumonia respiratory syncytial viral
Pneumonia viral
POEMS syndrome
Polyarteritis nodosa
Polyarthritis
Polychondritis
Polyglandular autoimmune syndrome type I
Polyglandular autoimmune syndrome type II
Polyglandular autoimmune syndrome type III
Polyglandular disorder
Polymicrogyria
Polymyalgia rheumatica
Polymyositis
Polyneuropathy
Polyneuropathy idiopathic progressive
Portal pyaemia
Portal vein embolism
Portal vein flow decreased
Portal vein pressure increased
Portal vein thrombosis
Portosplenomesenteric venous thrombosis
Post procedural hypotension
Post procedural pneumonia
Post procedural pulmonary embolism
Post stroke epilepsy
Post stroke seizure
Post thrombotic retinopathy
Post thrombotic syndrome
Post viral fatigue syndrome
Postictal headache
Postictal paralysis
Postictal psychosis
Postictal state
Postoperative respiratory distress
Postoperative respiratory failure
Postoperative thrombosis
Postpartum thrombosis
Postpartum venous thrombosis
Postpericardiotomy syndrome
Post-traumatic epilepsy
Postural orthostatic tachycardia syndrome
Precerebral artery thrombosis
Pre-eclampsia
Preictal state
Premature labour
Premature menopause
Primary amyloidosis
Primary biliary cholangitis
Primary progressive multiple sclerosis
Procedural shock
Proctitis herpes
Proctitis ulcerative
Product availability issue
Product distribution issue
Product supply issue
Progressive facial hemiatrophy
Progressive multifocal leukoencephalopathy
Progressive multiple sclerosis
Progressive relapsing multiple sclerosis
Prosthetic cardiac valve thrombosis
Pruritus
Pruritus allergic
Pseudovasculitis
Psoriasis
Psoriatic arthropathy
Pulmonary amyloidosis
Pulmonary artery thrombosis
Pulmonary embolism
Pulmonary fibrosis
Pulmonary haemorrhage
Pulmonary microemboli
Pulmonary oil microembolism
Pulmonary renal syndrome
Pulmonary sarcoidosis
Pulmonary sepsis
Pulmonary thrombosis
Pulmonary tumour thrombotic microangiopathy
Pulmonary vasculitis
Pulmonary veno-occlusive disease
Pulmonary venous thrombosis
Pyoderma gangrenosum
Pyostomatitis vegetans
Pyrexia
Quarantine
Radiation leukopenia
Radiculitis brachial
Radiologically isolated syndrome
Rash
Rash erythematous
Rash pruritic
Rasmussen encephalitis
Raynaud's phenomenon
Reactive capillary endothelial proliferation
Relapsing multiple sclerosis
Relapsing-remitting multiple sclerosis
Renal amyloidosis
Renal arteritis
Renal artery thrombosis
Renal embolism
Renal failure
Renal vascular thrombosis
Renal vasculitis
Renal vein embolism
Renal vein thrombosis
Respiratory arrest
Respiratory disorder
Respiratory distress
Respiratory failure
Respiratory paralysis
Respiratory syncytial virus bronchiolitis
Respiratory syncytial virus bronchitis
Retinal artery embolism
Retinal artery occlusion
Retinal artery thrombosis
Retinal vascular thrombosis
Retinal vasculitis
Retinal vein occlusion
Retinal vein thrombosis
Retinol binding protein decreased
Retinopathy
Retrograde portal vein flow
Retroperitoneal fibrosis
Reversible airways obstruction
Reynold's syndrome
Rheumatic brain disease
Rheumatic disorder
Rheumatoid arthritis
Rheumatoid factor increased
Rheumatoid factor positive
Rheumatoid factor quantitative increased
Rheumatoid lung
Rheumatoid neutrophilic dermatosis
Rheumatoid nodule
Rheumatoid nodule removal
Rheumatoid scleritis
Rheumatoid vasculitis
Saccadic eye movement
SAPHO syndrome
Sarcoidosis
SARS-CoV-l test
SARS-CoY-l test negative
SARS-CoV-l test positive
SARS-CoV-2 antibody test
SARS-CoV-2 antibody test negative
SARS-CoV-2 antibody test positive
SARS-CoV-2 carrier
SARS-CoY-2 sepsis
SARS-CoV-2 test
SARS-CoV-2 test false negative
SARS-CoV-2 test false positive
SARS-CoV-2 test negative
SARS-CoV-2 test positive
SARS-CoV-2 viraemia
Satoyoshi syndrome
Schizencephaly
Scleritis
Sclerodactylia
Scleroderma
Scleroderma associated digital ulcer
Scleroderma renal crisis
Scleroderma-like reaction
Secondary amyloidosis
Secondary cerebellar degeneration
Secondary progressive multiple sclerosis
Segmented hyalinising vasculitis
Seizure
Seizure anoxic
Seizure cluster
Seizure like phenomena
Seizure prophylaxis
Sensation of foreign body
Septic embolus
Septic pulmonary embolism
Severe acute respiratory syndrome
Severe myoclonic epilepsy of infancy
Shock
Shock symptom
Shrinking lung syndrome
Shunt thrombosis
Silent thyroiditis
Simple partial seizures
Sjogren's syndrome
Skin swelling
SLE arthritis
Smooth muscle antibody positive
Sneezing
Spinal artery embolism
Spinal artery thrombosis
Splenic artery thrombosis
Splenic embolism
Splenic thrombosis
Splenic vein thrombosis
Spondylitis
Spondyloarthropathy
Spontaneous heparin-induced thrombocytopenia syndrome
Status epilepticus
Stevens-Johnson syndrome
Stiff leg syndrome
Stiff person syndrome
Stillbirth
StiH's disease
Stoma site thrombosis
Stoma site vasculitis
Stress cardiomyopathy
Stridor
Subacute cutaneous lupus erythematosus
Subacute endocarditis
Subacute inflammatory demyelinating polyneuropathy
Subclavian artery embolism
Subclavian artery thrombosis
Subclavian vein thrombosis
Sudden unexplained death in epilepsy
Superior sagittal sinus thrombosis
Susac's syndrome
Suspected COVID-19
Swelling
Swelling face
Swelling of eyelid
Swollen tongue
Sympathetic ophthalmia
Systemic lupus erythematosus
Systemic lupus erythematosus disease activity index abnormal
Systemic lupus erythematosus disease activity index decreased
Systemic lupus erythematosus disease activity index increased
Systemic lupus erythematosus rashSystemic scleroderma
Systemic sclerosis pulmonary
Tachycardia
Tachypnoea
Takayasu's arteritis
Temporal lobe epilepsy
Terminal ileitis
Testicular autoimmunity
Throat tightness
Thromboangiitis obliterans
Thrombocytopenia
Thrombocytopenic purpura
Thrombophlebitis
Thrombophlebitis migrans
Thrombophlebitis neonatal
Thrombophlebitis septic
Thrombophlebitis superficial
Thromboplastin antibody positive
Thrombosis
Thrombosis corpora cavemosa
Thrombosis in device
Thrombosis mesenteric vessel
Thrombotic cerebral infarction
Thrombotic microangiopathy
Thrombotic stroke
Thrombotic thrombocytopenic purpura
Thyroid disorder
Thyroid stimulating immunoglobulin increased
Thyroiditis
Tongue amyloidosis
Tongue biting
Tongue oedema
Tonic clonic movements
Tonic convulsion
Tonic posturing
Topectomy
Total bile acids increased
Toxic epidermal necrolysis
Toxic leukoencephalopathy
Toxic oil syndrome
Tracheal obstruction
Tracheal oedema
Tracheobronchitis
Tracheobronchitis mycoplasmal
Tracheobronchitis viral
Transaminases abnormal
Transaminases increased
Transfusion-related alloimmune neutropenia
Transient epileptic amnesia
Transverse sinus thrombosis
Trigeminal nerve paresis
Trigeminal neuralgia
Trigeminal palsy
Truncus coeliacus thrombosis
Tuberous sclerosis complex
Tubulointerstitial nephritis and uveitis syndrome
Tumefactive multiple sclerosis
Tumour embolism
Tumour thrombosis
Type 1 diabetes mellitus
Type I hypersensitivity
Type III immune complex mediated reaction
Uhthoff's phenomenon
Ulcerative keratitis
Ultrasound liver abnormal
Umbilical cord thrombosis
Uncinate fits
Undifferentiated connective tissue disease
Upper airway obstruction
Urine bilirubin increased
Urobilinogen urine decreased
Urobilinogen urine increased
Urticaria
Urticaria papular
Urticarial vasculitis
Uterine rupture
Uveitis
Vaccination site thrombosis
Vaccination site vasculitis
Vagus nerve paralysis
Varicella
Varicella keratitis
Varicella post vaccine
Varicella zoster gastritis
Varicella zoster oesophagitis
Varicella zoster pneumonia
Varicella zoster sepsis
Varicella zoster virus infection
Vasa praevia
Vascular graft thrombosis
Vascular pseudoaneurysm thrombosis
Vascular purpura
Vascular stent thrombosis
Vasculitic rash
Vasculitic ulcer
Vasculitis
Vasculitis gastrointestinal
Vasculitis necrotising
Vena cava embolism
Vena cava thrombosis
Venous intravasation
Venous recanalisation
Venous thrombosis
Venous thrombosis in pregnancy
Venous thrombosis limb
Venous thrombosis neonatal
Vertebral artery thrombosis
Vessel puncture site thrombosis
Visceral venous thrombosis
VIth nerve paralysis
VIth nerve paresis
Vitiligo
Vocal cord paralysis
Vocal cord paresis
Vogt-Koyanagi-Harada disease
Warm type haemolytic anaemia
Wheezing
White nipple sign
XIth nerve paralysis
X-ray hepatobiliary abnormal
Young's syndrome
Zika virus associated Guillain Barre syndrome
A chronological listing from Mathew Crawford’s Rounding the Earth Newsletter of his analysis of the C19 shots spanning a year’s duration from November 2021 to 2022.
|
A chronological listing from Mathew Crawford’s Rounding the Earth Newsletter of his analysis of the development and official suppression of efficacious early treatment protocols making the C19 experiemental shots null and void from March 2021 to August 2022.
While the suppression of the free flow of information by corporate state arbiters of reality has reached previously unthinkable heights, there are many voices cutting through the mind-fog, presenting well-conceived critical analysis of how our world actually operates. A sampling of such open minds are presented in the following list of twelve books, including what has been learned by Doctors on-the-ground ministering to their patients needs. If the successes of early treatment protocols were acknowledged by government officials, so-called academic experts, and corporate state media organs, there would be no epidemic of the SARS-CoV-2 virus. From this, the Emergency Use Authorization would be null-and-void.
See Also: They Lied, People Died, Totality of Evidence.

The United States and Biological Warfare was published in 1998. Continuing from the Preface (emphasis added):
The U.S. Air Force had operational plans to use biological weapons in 1949 if the crisis surrounding the Berlin Blockade had led to general war, and later, during the Korean War, biological warfare was incorporated into the plans of the Strategic Air Command for general war, and into tactical plans for the U.S. Air Force in Europe. It is significant that this was the first time in modern military history that biological warfare was incorporated into doctrine as a weapons system. In addition, the United States had a technological capacity for the covert use of biological weapons, complete with a planning structure and operational capabilities.Top secret internal documents of the Chinese public health agency responsible for reporting any evidence of biological warfare in areas bordering Korea provide a coolly professional and balanced record, complete with sardonic observations on the sometime overreaction of the population to fears of germ warfare. When this material is placed beside information drawn from the medical and operational archives of the Chinese and North Korean armies in the field, a pattern of disease and delivery systems is observed consistent with American capabilities, and yet anomalous with local incidence of disease. These top secret internal medical and intelligence documents leave the impression that the Chinese were deadly serious in their efforts to figure out what was going on in a time of confusion, and were not attempting to manufacture a propaganda case. Significantly, very little of the archival material was used in 1952 in publicly making the case for germ warfare, and it has remained classified ever since. One can speculate that the Chinese and North Koreans, then and later, did not wish to share intelligence information that the Americans might use in assessing their experiments. In the aftermath of the Cold War, we have entered the Chinese and North Korean documents into the record.
From the U.S. archives, this book unfolds the hidden story of the extension of the limits of modern war to include the use of medical science, the most morally laden of sciences with respect to the sanctity of human life. Though the story of U.S. biological warfare follows a carefully concealed path, this path was in fact heavily traveled from World War II through the Korean War. Picking up from where World War II left off, through the early Cold War, the conflict in Korea quickly resurrected a heavily funded program with top-priority status that deeply involved the presidential office, the Department of Defense, and several other government departments and agencies, as well as the military services and the medical, scientific, academic, and corporate communities of the United States. A joint effort enlisted Great Britain and Canada in secret research and looked forward to incorporating a biological weapons system in NATO forces.
Working on an A-1 priority status, frequently under highest urgency orders, the leadership and rank and file of this network came together to develop bacteriological agents, munitions, and logistical support for the strategic and tactical use of bacteriological warfare in a general war plan aimed at the Soviet Union. At the midpoint of the Korean War, in December 1951, the U.S. secretary of defense ordered that “actual readiness be achieved in the earliest practicable time” for offensive use of biological weapons. Within weeks, the chief of staff of the U.S. Air Force reported that such capabilities “are rapidly materializing.” It was shortly after these secret communications had passed between the top U.S. generals that the North Korean and Chinese armies charged the United States with beginning a large-scale biological warfare experiment in Korea. The U.S. secretary of state flatly denied the accusation. Both sides maintain their positions to this day. Our research has been directed to investigating and resolving this contradiction.
The momentum of and mood surrounding U.S. bacteriological development, the level of concern over the need for human experiment, and the crisis atmosphere of the time—a time when the United States military had suffered “a series of disasters unequaled in our country’s history” (Appleman, Disaster in Korea, p. 5)—compels the historian to ask, without prejudging the answer, why U.S. forces would not use bacteriological warfare in Korea. What military, political, or moral restraints applied in that moment of ideological and political passion and of military crisis?
Questions of moral scruple about using “public health and preventive medicine in reverse” largely disappeared in an early post-World War II decision that came as close to a pact with the devil as any in U.S. political or military history. On the initiative of the service chiefs, the United States granted immunity to a group of Japanese war criminals (who had conducted biological warfare experiments on Chinese cities and had murdered at least three thousand prisoners of war, including some Americans, in the course of “scientific” germ war tests) in return for their cooperation in sharing their knowledge of biological warfare. The Japanese program and the U.S. deal remained one of the best-kept official secrets of the two countries for more than thirty-five years. The declassified documentary record remains conspicuously silent on how the Japanese program was integrated into the American.
Despite silence on the Japanese connection, gradual declassification over the past twenty years has revealed an expanding picture of policy, action, and motives about biological warfare. This book is an attempt to fill in this picture by bringing together our research in the United States, China, Japan, Britain, Canada, and Continental Europe, and the labors of others who preceded us. Our hope is to contribute to the historical understanding of a moment of crisis when the limits of modern war expanded into a fundamentally new form of violence.
The chapter on World War II Origins describes how bacteriological warfare developed:
p.29:
Just as the chemical industry had lobbied for an active chemical warfare policy during the interwar years, the pharmaceutical industry was conspicuous in promoting bacteriological warfare development during World War II. George W. Merck (head of the pharmaceutical giant Merck & Co.) was recruited by the Roosevelt administration to head the civilian War Research Service (WRS) Committee (successor to the Branch of War Research in Chemistry). Created in March 1942, the WRS Committee was to coordinate biological warfare work.p.31:
Begun with an initial grant of $250,000, modest by wartime standards, the biological warfare program quickly grew to be one of the largest wartime scientific projects in American history, second only to the Manhattan Project, which had created the atomic bomb. Granted top-priority status, the program employed approximately four thousand people by the end of the war. The center of activity was the Special Projects Division of the Chemical Warfare Service and its new research and development center located at Camp Detrick, Maryland.Camp Detrick was established in April 1943 when it became obvious that the Chemical Warfare Service’s Edgewood Arsenal, also in Maryland, could not handle the expanded activity. By the end of that year, Detrick was well into large-scale research.... The Detrick scientists cast a wide experimental net. They studied anthrax, brucellosis (undulant fever), botulinus toxin, plague, ricin, southern blight of grains, potatoes, and sugar beets (Sclerotium rolfoil), late blight, late blast, brownspot of rice, plant growth inhibitors, rinderpest, glanders and melioidosis (pseudoglanders), tularemia (rabbit fever), mussel poisoning, coccidioidomycosis, rickettsia, psittacosis, neurotropic encephalitis, Newcastle disease, and fowl plague. They monitored independent studies of cholera, rinderpest, and foot-and-mouth disease, and a Canadian study of typhus. They then got involved in the project on ricin, which involved Johns Hopkins, Procter and Gamble, and the British at Suffield, Alberta. By the end of 1943, the team working with ricin had concluded that it was as deadly as botulinus and cheaper and easier to produce. Beyond these projects, other agents were investigated. (Merck reports that all potential agents were evaluated.) The first to receive concentrated attention at Detrick were anthrax and botulinus toxin.
The book’s Conclusion distills how the executive branch of the federal government integrated biological warfare into the US military arsenal.
p.186:
As far as the Joint Chiefs were concerned, biological weapons could be employed from the outset of war at the discretion of the president. This position was not formalized by the National Security Council until March 1956. However, it is clear that biological warfare had been assimilated by the U.S. military and had become a significant, even central, element in U.S. military thinking and practice by 1952; they expected to have a mature operational plan in place within two years. Lingering doubts pertained mainly to the effectiveness of current methods for delivering available bacterial agents....p.198:
What unravels is the story of how the newly empowered U.S. Defense Department revived and funded a broad coalition of military, private, and public-sector interests from World War II to implement a crash program in biological warfare. Its mission was to achieve emergency operational readiness in the shortest possible time. Support for the program was driven by the mixed motives of ideology, fear, racism, power, profit, and the visceral excitement of an opportunity at the new frontiers of science and war.
Hello. My name is Dr. Richard Fleming. I’m a physicist, nuclear cardiologist, and an attorney. For the last 53 years of my life, I’ve been involved in scientific research. Like many of you, in 2019, my world changed. As all of us became painfully aware of a new virus spreading around the world, and with the advent of 2020, a pandemic that would shut down all nations, all travel and all economies, I began an investigation looking at the cause of this disease and treatments.
It’s fair to say that in 1994, I introduced at the American Heart Association meetings, the very theory that explained how viruses like SARS-CoV-2 could produce a disease like COVID-19. I also developed a method called the Fleming Method to measure what’s going on inside the body so that we could determine how severe the disease was and which treatments were working.
In the process of carrying out that investigation, I like you, asked some very fundamental questions. The primary one being, Where did this virus come from? And, more importantly, Was it naturally occurring or was it manmade?
In a book I’ve written called Is COVID 19 a Bioweapon? A Scientific and Forensic Investigation, I’m going to share with you the information I’ve learned. I’m going to begin by explaining what Gain-of-Function is: the ability of scientists and researchers to take a virus and make it more infective and more harmful.
More importantly than that, we’re going to look at a series of papers that were published in the medical and scientific research literature that shows exactly how this virus was made and by whom. We’re going to look at the patents that were given and who benefits from those patents. And we’re going to look and find the sources of funding. Who paid for the development of SARS-CoV-2 that would produce the disease, COVID-19, shut down the planet, and who’s responsible for telling you that treatments don’t work and that vaccines do.
We’re going to link up these people and show you that the very people who helped fund and develop and launch this bioweapon are the very same people that are telling you there are no treatments, and you must use this vaccine. As we go through this book, I’m going to share some astonishing information, all of which you can validate and verify on your own; presuming they haven’t removed it from the internet. That being said, I’ve saved the original sources and shared them with the publisher and attorneys so that when it comes time to address these crimes against humanity, the record will still be intact.
This is Dr. Richard Fleming. I hope you enjoy reading this book and sharing the information with your friends and family. The questions that you’ve been asking, you have a right to get the answers to, and this book provides those answers.
The following listing is published in Chapter 3, The Paper Trail of the US Funding for Gain-of-Function Research of Dr. Richard M. Fleming’s 2021 book, Is COVID-19 a Bioweapon? It is the compilation of some of the money trail paid by agencies in the United States Executive Branch—from US taxpayer dollars—to EcoHealth Alliance Inc. In the below links, other names for EcoHealth Alliance Inc. are: “WILDLIFE TRUST”, “WILDLIFE TRUST INC”, “WILDLIFE TRUST INC.”, and “WILDLIFE TRUST INCORPORATED”.
The above graphic shows
All Fiscal Years spending, from 2008 into 2023, of US Federal
Government funding EcoHealth Alliance Inc.
Defense Threat Reduction Agency (DOD)
2015 Award ID HDTRA115C0041 for the amount of $2,217,037.00
2016 Award ID HDTRA115C0041 for the amount of $2,262,641.00
https://www.usaspending.gov/award/CONT_AWD_HDTRA115C0041_9700_-NONE-_-NONE-
Defense Threat Reduction Agency (DOD)
2017 Award ID HDTRA11710037 for the amount of $721,249.00
2018 Award ID HDTRA11710037 for the amount of $883,274.00
https://www.usaspending.gov/award/ASST_NON_HDTRA11710037_9761
“Scientific Research - Combating Weapons of Mass Destruction” no date
Defense Threat Reduction Agency (DOD)
2019 Award ID HDTRA11910033 for the amount of $998,437.00
2020 Award ID HDTRA11910033 for the amount of $3,990,550.00
https://www.usaspending.gov/award/ASST_NON_HDTRA11910033_9761
Defense Threat Reduction Agency (DOD)
2013 Award ID HDTRA113C0029 for the amount of $1,371,611.00
2014 Award ID HDTRA113C0029 for the amount of $957,145.00
2015 Award ID HDTRA113C0029 for the amount of $-103,622.00
https://www.usaspending.gov/award/CONT_AWD_HDTRA113C0029_9700_-NONE-_-NONE-
Department of Defense (DOD)
2014 Award ID HDTRA11410029 (#1) for the amount of $992,699.00
2015 Award ID HDTRA11410029 (#1) for the amount of $978,784.00
2016 Award ID HDTRA11410029 (#1) for the amount of $970,536.00
https://www.usaspending.gov/award/ASST_NON_HDTRA11410029_9700
Defense Threat Reduction Agency (DOD)
2017 Award ID HDTRA11410029 (#2) for the amount of $996,147.00
2018 Award ID HDTRA11410029 (#2) for the amount of $998,193.00
https://www.usaspending.gov/award/ASST_NON_HDTRA11410029_9761
Defense Threat Reduction Agency (DOD)
2020 Award ID HDTRA12010016 for the amount of $4,912,818.00
https://www.usaspending.gov/award/ASST_NON_HDTRA12010016_9761
Defense Threat Reduction Agency (DOD)
2017 Award ID HDTRA11710064 for the amount of $782,330.00
2018 Award ID HDTRA11710064 for the amount of $2,203,917.00
2019 Award ID HDTRA11710064 for the amount of $1,995,247.00
2020 Award ID HDTRA11710064 for the amount of $1,509,531.00
https://www.usaspending.gov/award/ASST_NON_HDTRA11710064_9761
Defense Threat Reduction Agency (DOD)
2020 Award ID HDTRA12010018 for the amount of $4,995,106.00
https://www.usaspending.gov/award/ASST_NON_HDTRA12010018_9761
Uniformed Services University of the Health Sciences (DOD)
2020 Award ID HU00012010031 for the amount of $1,360,002.00
https://www.usaspending.gov/award/ASST_NON_HU00012010031_97HW
Defense Threat Reduction Agency (DOD)
2020 Award ID HDTRA12010029 for the amount of $2,956,309.00
https://www.usaspending.gov/award/ASST_NON_HDTRA12010029_9761
National Institutes of Health-NIH (HHS)
2007 Award ID K08AI067549 for the amount of $130,950
2009 Award ID K08AI067549 for the amount of $180,944
2010 Award ID K08AI067549 for the amount of $130,950
https://www.usaspending.gov/award/ASST_NON_K08AI067549_7529
National Institutes of Health-NIH (HHS)
2007 Award ID R56TW009502 for the amount of $300,000.00
https://www.usaspending.gov/award/ASST_NON_R56TW009502_7529
National Institute of Allergy and Infectious Diseases (HHS-NIH)
2014 Award ID R01AI110964 for the amount of $666,442.00
2015 Award ID R01AI110964 for the amount of $630,445.00
2016 Award ID R01AI110964 for the amount of $611,090.00
2017 Award ID R01AI110964 for the amount of $597,112.00
2018 Award ID R01AI110964 for the amount of $581,646.00
https://www.usaspending.gov/award/ASST_NON_R01AI110964_7529
CDC Office of Acquisition Services (HHS)
2011 Award ID HHSD2002011M41641P for the amount of $59,740.00
2013 Award ID HHSD2002011M41641P for the amount of $45,000.00
2016 Award ID HHSD2002011M41641P for the amount of $-5,446.00
https://www.usaspending.gov/award/CONT_AWD_HHSD2002011M41641P_7523_-NONE-_-NONE-
National Institutes of Health (HHS)
2008 Award ID R01AI079231 for the amount of $534,989.00
2009 Award ID R01AI079231 for the amount of $535,156.00
2010 Award ID R01AI079231 for the amount of $480,423.00
2011 Award ID R01AI079231 for the amount of $510,005.00
2012 Award ID R01AI079231 for the amount of $518,980.00
https://www.usaspending.gov/award/ASST_NON_R01AI079231_7529
NIH National Institute of Allergy and Infectious Diseases (NIAID) (HHS)
2020 Award ID U01AI151797 for the amount of $1,546,744.00
https://www.usaspending.gov/award/ASST_NON_U01AI151797_7529
Department of Health and Human Services (HHS)
2020 Award ID U01AI153420 for the amount of $580,858.00
https://www.usaspending.gov/award/ASST_NON_U01AI153420_7529
National Science Foundation (NSF)
2017 Award ID 1714394 for the amount of $138,000.00
2020 Award ID 1714394 for the amount of $-40,250.00
https://www.usaspending.gov/award/ASST_NON_1714394_4900
Division of Environmental Biology (NSF)
2010 Award ID 1015791 for the amount of $29,109.00
2012 Award ID 1015791 for the amount of $13,948.00
2013 Award ID 1015791 for the amount of $14,293.00
2014 Award ID 1015791 for the amount of $14,652.00
https://www.usaspending.gov/award/ASST_NON_1015791_4900
National Science Foundation (NSF)
2012 Award ID 1257513 for the amount of $22,890.00
https://www.usaspending.gov/award/ASST_NON_1257513_4900
Division of Environmental Biology (NSF)
2010 Award ID 955897 for the amount of $99,611.00
2011 Award ID 955897 for the amount of $98,673.00
2012 Award ID 955897 for the amount of $99,919.00
2013 Award ID 955897 for the amount of $98,992.00
2014 Award ID 955897 for the amount of $99,926.00
https://www.usaspending.gov/award/ASST_NON_0955897_4900
National Science Foundation (NSF)
2006 Award ID 0622391 for the amount of $503,291.00
2008 Award ID 0622391 for the amount of $428,794.00
https://www.usaspending.gov/award/ASST_NON_0622391_4900
National Science Foundation (NSF)
2008 Award ID 0826779 for the amount of $468,673.00
https://www.usaspending.gov/award/ASST_NON_0826779_4900
Office of Health Affairs Acquisition Division (DHS)
2016 Award ID HSHQDC16C00113 for the amount of $271,272.00
2017 Award ID HSHQDC16C00113 for the amount of $327,782.00
2018 Award ID HSHQDC16C00113 for the amount of $406,902.00
https://www.usaspending.gov/award/CONT_AWD_HSHQDC16C00113_7001_-NONE-_-NONE-
Science and Technology Acquisition Division (DHS)
2017 Award ID 70RSAT18CB0031001 for the amount of $413,761.00
2018 Award ID 70RSAT18CB0031001 for the amount of $246,770.00
2019 Award ID 70RSAT18CB0031001 for the amount of $40,052.00
https://www.usaspending.gov/award/CONT_AWD_70RSAT18CB0031001_7001_-NONE-_-NONE-
Department of Agriculture (USDA)
2009 Award ID 09-7100-0206-CA for the amount of $100,001.00

Animal and Plant Inspection Service (USDA)
2007 Award ID 07-7100-0237-CA for the amount of $403,700.00
https://www.usaspending.gov/award/ASST_NON_07-7100-0237-CA_12K3
U.S. Fish & Wildlife Services (DOI)
2012 Award ID F12AP01117 for the amount of $44,499.00
https://www.usaspending.gov/award/ASST_NON_F12AP01117_1448
U.S. Fish & Wildlife Services (DOI)
2014 Award ID F14AP00269 for the amount of $29,988.00
https://www.usaspending.gov/award/ASST_NON_F14AP00269_1448
Office of Acquisition and Grants-Reston (DOI)
2004 Award ID ING04ERSA0526 for the amount of $16,000.00
2005 Award ID ING04ERSA0526 for the amount of $15,000.00
2006 Award ID ING04ERSA0526 for the amount of $10,000.00
2007 Award ID ING04ERSA0526 for the amount of $10,000.00
2008 Award ID ING04ERSA0526 for the amount of $10,000.00
https://www.usaspending.gov/award/CONT_AWD_ING04ERSA0526_1434_-NONE-_-NONE-
Department of the Interior (DOI)
2011 Award ID G05AC00002 for the amount of $-22,512.00
https://www.usaspending.gov/award/ASST_NON_G05AC00002_1434
Selected monumental research and critical analysis by Katherine Watt from her publication, Bailiwick News. (I prefer studying a more compressed text-only bullet listing of someone’s research than the tedious way one must sift prior posts inside the Substack archive format.)
Many, many, many souls are engaged in ending the blinding darkness of fear from which can proceed, life-nurturing support for the human project’s creative evolutionary adaption into our post-industrial-mind epoch.
Listed below are 17,700+ physicians and scientists who have stood fast in their commitment and loyalty to the Hippocratic Oath regardless of the consequences to their careers and livelihoods, as well as medical professionals, scientists, public health professionals, and journalists who have stood up for genuine transparency of the data relied upon by the FDA to license COVID-19 vaccines.
In addition to the following, people referenced throughout this essay constitute a minute fraction of those around the world working in a multitude of areas to carry on the work of the ancestors to lay bare the Domination System and participate in remembering how
|
“
|
Critics make the amateurish assumption that the Great Reset is the brainchild of Schwab. There is nothing theoretically new about many of the Great Reset’s underlying principles. Technologies such as 5G telecommunications, robotics and artificial intelligence, data collection and surveillance, block chain applications, biotechnology and genetic engineering and transhumanist visions were already becoming exponentially more complex and sophisticated....
It may surprise many that since its inception in 1971 the WEF has achieved little. Despite the enormity of its public face to the world, by itself the Forum is a lot of smoke and mirrors, a climax of human hubris and self-deception. Left to itself, it is a rather lame institution. Schwab himself has stated that his organization’s sole purpose is to initiate “dialogue between stakeholders” and doesn’t engage in negotiations for treaties and policy decisions. “Elites have always existed,” Schwab once stated, “We bring together people of influence, and we hope they use their influence in a positive way.” The Forum is largely a huge clearing house, which internalizes enormous amounts of analytical reports, public and private symposia, geopolitical analyses and scenario exercises from a wide network of governmental, multilateral organizations, transnational corporations and financial firms, banks, think tanks, NGOs and no doubt intelligence entities and elitist institutions such as Bill and Melinda Gates Foundation, the Tavistock Institute, the Trilateral Commission, Council on Foreign Relations, Bilderberg and many more. It has never truly succeeded in anything monumental other than serving as a premier incubator for the Davos Men, corporate multinational and financial elite and their well funded think tanks and NGOs, to network behind closed doors and conjure new ways to preserve and advance a post-capitalist technological agenda without overly disrupting the neoliberal agenda upon which these entities depend. Yet it is in the WEF’s DNA to advance a template for socio-economic progress defined by a technologically driven regime that will not trigger earthquakes through the ruling elite class.
More worrisome is the younger generation who willingly and eagerly become incentivized by the market value of infinite technological innovations and progress despite its egregious applications for surveillance, social restructuring and behavior modification. Corporate techno-nerds pursue means to artificially mechanize human biology and dream of a transhumanist future populated by human cyborgs. The miracles of CRISPR engineering to more easily manipulate the genome of every species offers the technological future infinite Promethean possibilities....
The globalists’ adrenaline rush during the past years of the pandemic has been an effort to shatter the public’s self-awareness, to squash individuality and dumb down critical thought. Viewed from this perspective, social movements such as the New Woke, environmentalism as an ideology created by the elites’ Green Deal agendas, and gender insanity were likely very predictable now that we have seen them being co-opted by the same Great Reset conductors. They are synonymous with a system that needs to shatter the public’s conscious self-awareness and replace democracy with idiocracy for mass consumption. This includes abolishing public control over social media networks, as witnessed by the US Democrat and EU governments’ and their woke lackeys’ backlash against Elon Musk’s purchase of Twitter.
—Gary Null,
The Great Reset and the Post-Capitalist Revolution, prn.live 19 Dec 2022
|
From Robert Kennedy, Jr.’s Dedication at the beginning of The Real Anthony Fauci:
I dedicate this book to that battle-hardened cadre of heroic scientists and physicians who have risked their careers, their livelihoods, and their reputations to champion evidence-based science and ethical medicine. By steadfastly prioritizing truth, the welfare of their patients, and the cause of public health above their own career ambitions, these brave men and women have succeeded, at great cost, in preserving their own integrity. They may one day restore from shame the shattered souls of the medical profession and the scientific establishment. Each of these individuals has emerged as a voice of sanity and a symbol of clarity and truth to those idealists across the globe who love democracy and resist the rising medical authoritarianism. Thanks to all of you for inspiring me with your character, your courage, your brilliant insights, and your passion for empiricism and critical thinking.
The Heroic Healers Honor Roll
There is a much larger retinue of thousands of lesser-known front-line medical professionals and PhD. researchers who have also chosen to wager everything on their commitment to their patients, to uncorrupted scientific inquiry, and to the opposition to authoritarian COVID policies. Many of them have battled unheralded in the trenches for decades. Each one of them has endured various intensities of vilification, excommunication, delicensing, and censorship by the Pharma cartel’s captive regulators, its corrupt medical associations, its media and social media allies and medical journals, and its government-sponsored fact checkers. They have weathered derision, gaslighting, scapegoating, retractions, career and reputational injuries, and financial ruin, to protect their patients, and nurture truth. My apologies to all of you whom I have necessarily omitted due to space restrictions but who belong on this Honor Roll. I regret that the only consolation for your sacrifices may be a clear conscience.
|
Dr. Robin Armstrong
Dr. Cristian Arvinte Dr. David Ayoub Dr. Alan Bain Dr. Richard Bartlett Dr. Cammy Benton Dr. Robert Berkowitz Dr. Andrew Berry Dr. Harvey Bialy Dr. Thomas Borody Dr. Joseph Brewer Dr. Kelly Brogan Dr. David Brownstein Dr. Adam Brufsky Dr. Zach Bush Dr. Dolores Cahill Dr. Teryn Clarke Dr. Tom Cowan Dr. Andrew Cutler Dr. Roland Derwand Dr. Joyce Drayton Dr. Peter Duesberg Dr. Alieta Eck Dr. John Eck Dr. Richard Eisner Dr. Christopher Exley Dr. George Fareed Dr. Angelina Farella Dr. Richard Fleming Dr. Ted Fogarty Dr. Silvia N.S. Fonseca Dr. C. Stephen Frost Dr. Michael Geier Dr. Charles Geyer |
Dr. Simone Gold
Dr. Gary Goldman Dr. Russell Gonnering Dr. Karladine Graves Dr. Kenneth Gross Dr. Sabine Hazan Dr. Kristin Held Dr. H. Thomas Hight Dr. LeTrinh Hoang Dr. Douglas Hulstedt Dr. Suzanne Humphries Dr. Stella Immanuel Dr. Michael Jacobs Dr. Tina Kimmel Dr. Lionel H. Lee Dr. Sin Han Lee Dr. John Littell Dr. Ivette Lozano Dr. Douglas Mackenzie Dr. Carrie Madej Dr. Marty Makary Dr. Harpal Mangat Dr. Ben Marble Dr. David E. Martin Dr. John E. McKinnon Dr. Shira Miller Dr. Kari Mullis Dr. Liz Mumper Dr. Eileen Natuzzi Dr. James Neuenschwander Dr. Hooman Noorchashm Dr. Jane Orient Dr. Tetyana Obukhanych Dr. Ramin Oskoui |
Dr. Larry Palevsky
Dr. Vicky Pebsworth Dr. Don Pompan Dr. Brian Procter Dr. Chad Prodromos Dr. Jean-Jacques Rajter Dr. Juliana Cepelowicz Rajter Dr. C. Venkata Ram Dr. David Rasnick Dr. Salete Rios Dr. Michael Robb Dr. Rachel Ross Dr. Moll Rutherford Dr. Ed Sarraf Dr. Martin Scholz Dr. Bob Sears Dr. Christopher Shaw Dr. Marilyn Singleton Dr. Kenneth Stoller Dr. Kelly Sutton Dr. Sherri Tenpenny Dr. Paul Thomas Dr. James Tumlin Dr. Brian Tyson Dr. Michelle Veneziano Dr. Kelly Victory Dr. Elizabeth Lee Vliet Dr. Craig Wax Dr. Rachel West Dr. James Lyons-Weiler Dr. Alexandre Wolkoff Dr. Vicki Wooll Dr. Bob Zajac Dr. Andrew Zimmerman |
From PHYSICIANS DECLARATION - GLOBAL COVID SUMMIT, International Alliance of Physicians and Medical Scientists:
As of 8am ET on 1/18 over 17,000 doctors & scientists have signed the Rome Declaration
WE, THE PHYSICIANS OF THE WORLD, united and loyal to the Hippocratic Oath, recognizing the imminent threat to humanity brought forth by current Covid-19 policies, are compelled to declare the following:
WHEREAS, after 20 months of research, millions of patients treated, hundreds of clinical trials performed and scientific data shared, we have demonstrated and documented our success and understanding in combating COVID-19;
WHEREAS, in considering the risks vs. benefits of major policy decisions, thousands of physicians and medical scientists worldwide have reached consensus on three foundational principles;
NOW THEREFORE, IT IS:
RESOLVED, THAT HEALTHY CHILDREN SHALL NOT BE SUBJECT TO FORCED VACCINATION (view supporting evidence)
RESOLVED, THAT NATURALLY IMMUNE PERSONS RECOVERED FROM SARS-CoV-2 SHALL NOT BE SUBJECT TO ANY RESTRICTIONS OR VACCINE MANDATES (view supporting evidence)
RESOLVED, THAT ALL HEALTH AGENCIES AND INSTITUTIONS SHALL CEASE INTERFERING WITH PHYSICIANS TREATING INDIVIDUAL PATIENTS (view supporting evidence)
RECOMMENDED LEGISLATIVE OR EXECUTIVE ACTION:
We believe that violating any of these three principles unnecessarily and directly risks death to our citizens. We hereby recommend the leaders of states, provinces and nations legislate or take executive action to prohibit the three practices described above.
IN WITNESS WHEREOF, the undersigned has signed this Declaration.
From Public Health and Medical Professionals for Transparency:
This nonprofit, made up of public health professionals, medical professionals, scientists, and journalists exists solely to obtain and disseminate the data relied upon by the FDA to license COVID-19 vaccines. The organization takes no position on the data other than that it should be made publicly available to allow independent experts to conduct their own review and analyses. Any data received will be made public on this website.
Four days after the Pfizer vaccine was approved for ages 16+, we submitted a Freedom of Information Act Request to the FDA for all of the data within Pfizer’s COVID-19 vaccine biological product file. We have now sued the FDA for not releasing the data. See Court documents and productions of Pfizer’s documents from the FDA.
The following list was replicated from https://phmpt.org/members/ in November 2022. As of 16 Sep 2023, there are 5,455+ Members.




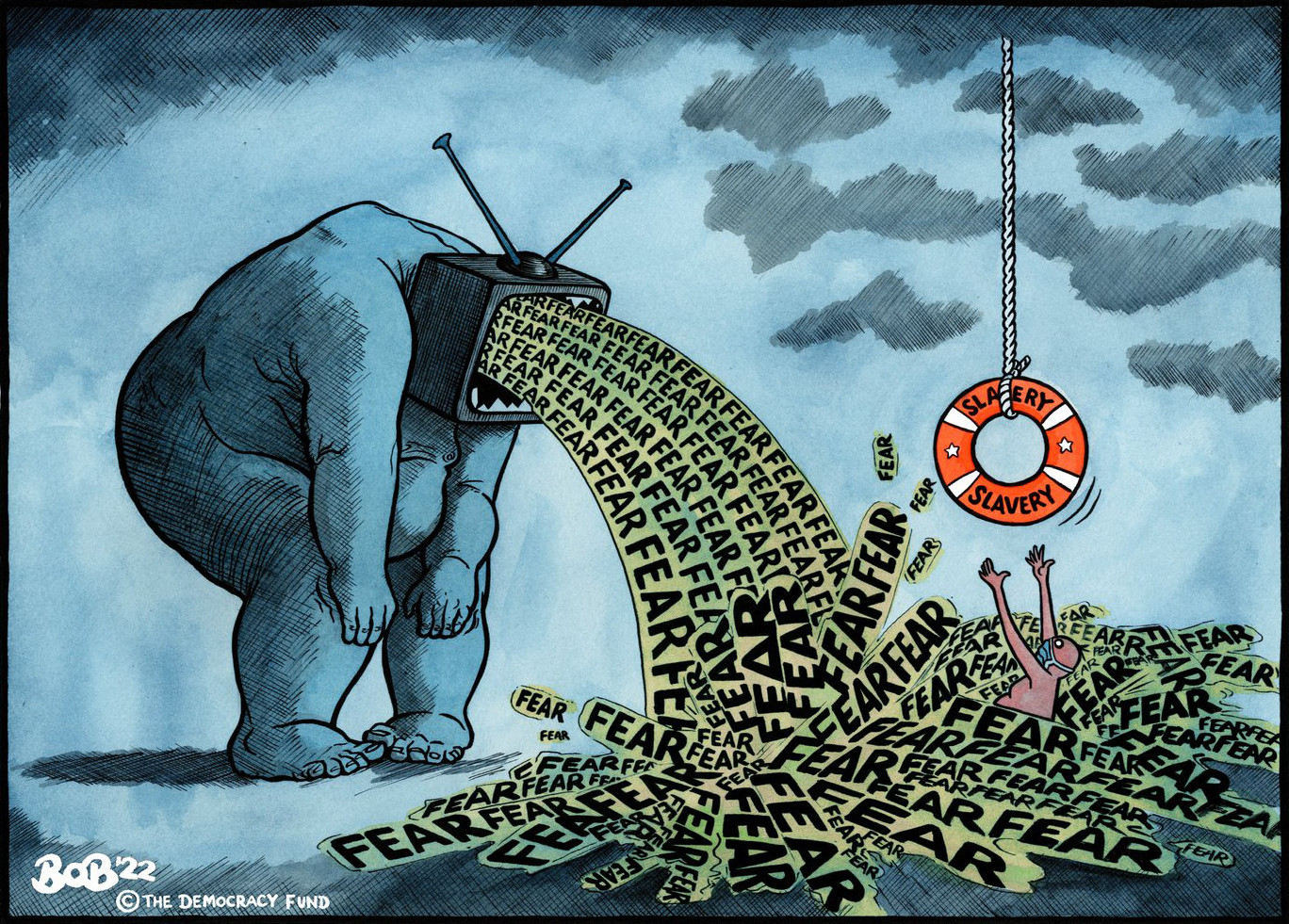




























{kind=link}